- U.S. States Warm, But Not As Expected

- Rovner Recaps Medicaid Cuts’ Impact on Hospitals and Fields Caller Questions on Affordability

- CMS proposes mandatory hospital-bundled model for joint replacements
- CMS proposes mandatory hospital-bundled model for joint replacements
- CMS proposes mandatory hospital-bundled model for joint replacements
- CMS pitches 2.4% hospital pay bump, mandatory joint replacement model: 7 things to know
- CMS pitches 2.4% hospital pay bump, mandatory joint replacement model: 7 things to know
- Mayo Clinic enhances imaging test with AI
- Christus Health to open Texas multi-specialty clinic
- CMS proposes extension of prior authorization rule to cover drugs: 6 notes
- Penn Medicine, Epic lean into EHR ‘nudges’
- AdventHealth breaks ground on $27M freestanding ER
- Henry Ford hospital strike enters 7th month: 6 notes
- Texas launches rural hospital leadership academy
- Children’s Minnesota staff email account compromised
- UHS’ CEO-to-worker pay ratio over the past 5 years
- 11 things to know about the uninsured population: KFF
- Medicaid’s consistency problem in dentistry
- Dental groups seek $600M+ in FY 2027 federal budget: 5 notes
- Missouri dental school grows student body by 33% to combat dentist shortages
- Prior authorization by the numbers: 10 stats that show the strain
- The Trump Administration Is Seeking Federal Workers’ Sensitive Medical Data. That’s Raising Alarms.

- 5 new university programs tackling behavioral health workforce gaps
- How Mount Sinai is transforming its revenue cycle
- Hospital revenue cycle teams evolve as AI ‘arms race’ heats up
- Texas Children’s gets $5M gift for behavioral health services
- Cardiology malpractice cases by the numbers
- Texas Children’s receives $5M estate gift for behavioral health
- CMS proposes 2.4% hospital pay increase, nationwide mandatory model rollout
- Which physician specialty is most likely to have a salaried paycheck?
- 20+ dental education updates to know from Q1
- Proposed CMS rule would set prior auth deadlines for drugs
- The best orthopedic ASCs in the West: US News
- 4 clinics closing after physician owner sentenced for selling recalled medical devices as new
- The hospitals, health systems cutting jobs in 2026
- VA program deploys 700+ VR ‘mental wellness’ kits
- The cost of private equity firms owning residential SUD facilities: 4 things to know
- 10 highest, lowest-paying physician specialties
- Independent GI practices shrinks as reimbursements fall 38% over a decade
- HHS, after legal setback, updates ACIP charter to put more emphasis on vaccine safety
- HHS, after legal setback, updates ACIP charter to put more emphasis on vaccine safety
- New York system to open $12M outpatient imaging center
- Costco Recalls Cookies Over Missing Nut Allergy Warning
- CDC Pauses Release of COVID Vaccine Effectiveness Study
- Pharma company withdraws FDA application amid White House autism treatment push
- UCI Health reverses layoffs of 7 quality improvement workers
- Endoscopy at scale: The reprocessing best practices separating high-performing teams

- 30 hospitals closing departments or ending services
- Demand Surge Leads to Shortages of Estrogen Patches
- What to know about the fastest-growing DSO
- 4 DSOs making headlines
- Statement Regarding Staff No-Action Letter to Bank of England
- Op-ed: Administrative fragility is costing healthcare more than we think
- Alaska city opens addiction treatment microunit program
- Title X Funding Restored, but New Rules Raise Concerns
- Function Health acquires mobile healthcare platform Getlabs to provide members with at-home lab tests
- The Healthcare Burnout Backlash (pt 3): How Workflow Redesign Is Helping Healthcare Organizations Offset Staffing Shortages
: How Workflow Redesign Is Helping Healthcare Organizations Offset Staffing Shortages")
- The Healthcare Burnout Backlash (pt 3): How Workflow Redesign Is Helping Healthcare Organizations Offset Staffing Shortages
- BD Announced Application of CE Mark for the Liverty TIPS Stent Graft

- BD Announced Application of CE Mark for the Liverty TIPS Stent Graft
- Blackstone and TPG Complete Acquisition of Hologic; Names New CEO
- Blackstone and TPG Complete Acquisition of Hologic; Names New CEO
- Endospan Receives FDA Approval for the NEXUS Aortic Arch Stent Graft System
- Endospan Receives FDA Approval for the NEXUS Aortic Arch Stent Graft System
- InVera Medical Receives FDA Clearance for Non-Thermal Chronic Venous Disease Device

- InVera Medical Receives FDA Clearance for Non-Thermal Chronic Venous Disease Device
- Starting material sourcing bottlenecks increase US drug shortage risks: report
- Novartis cuts 114 more jobs at New Jersey HQ as restructuring rolls on
- Charles River flows into Boston to help AHA bridge cardiovascular health divide
- Your Brain Cares If Your Plant-Based Diet Is Unhealthy, Researchers Report
- Your Neighborhood Might Help Make You Old Before Your Time
- Heavy 'Forever Chemical' Exposure Before Birth Increases Childhood Asthma Risk, Study Finds
- High-Tech Magnets Offer New Hope for Veterans Battling Combat PTSD
- Early Diagnosis Key To ADHD Child's Academic Success, Study Finds
- Study Reveals Who Americans Think Should Pay for Elder Care
- Envision hires ConcertAI, IQVIA alum Nick Jones as its med comms president
- The top 10 pharma R&D budgets of 2025
- Watch: As AI Makes More Health Coverage Decisions, the Risks to Patients Grow

- For Many Patients Leaving the ICU, the Struggle Has Only Just Begun

- Bial launches ‘Dialogues with Parkinson’s’ campaign aimed at identifying early symptoms
- Novartis pumps up community health footprint to tackle heart disease and cancer
- Abbott survey finds ‘information overload, confusion and cost’ affecting health choices in US
- FDA accuses Amneal, BioCorRx of producing ‘false and misleading’ drug promos
- North Carolina provider launches mobile opioid treatment unit
- U of Pittsburgh debuts online infant mental health certificate
- Emerging DSO lands Ohio partnership
- Heartland Dental added 5 de novos in March
- Florida International U, medical school land $30M gift for medical center
- Stanford Health, Alameda Health System partner to support California hospital
- The states with the highest, lowest migration rate of dentists since 2019
- What the Health? From KFF Health News: Abortion Pills, the Budget, and RFK Jr.

- Specialty DSO eyes new growth levers after entering several states
- Hospital M&A roars back to life in Q1 2026; Operating performances fray in February
- Epic rolls out health alerts to flag rising rates of illness at the county level
- Fierce Pharma Asia—Takeda-Denali split-up; Merck, Zhifei's revised deal; Shionogi's made-in-US plan
- Brain Scans Reveal How Psychedelics Change Perception
- Benefits leaders report increased operational, financial costs amid 'digital health vendor sprawl': Solera survey
- Vanda initiates study of motion sickness drug Nereus in GLP-1 users
- Judge Allows Abortion Pill, Mifepristone, To Continue Being Mailed for Now
- Bangladesh Measles Outbreak Kills 100+ Kids, Emergency Shots Begin
- Regulatory burdens continue to mount for physician practices
- Medicare navigation company Chapter banks $100M series E funding round
- Hair Growth Product, Tuymec Minoxidil Hair Growth Kits, Recalled Over Child Poisoning Risk
- Garda snaps up Assertio and chemo infection treatment Rolvedon in $125M deal
- AbbVie challenges 'outdated' 340B drug discount program guidance in new lawsuit
- AbbVie challenges 'outdated' 340B drug discount program guidance in new lawsuit
- Eli Lilly launches oral GLP-1 drug across US through Lilly Direct, telehealth providers
- Humana, Noom and Welldoc team up with b.well to expand health data access as part of CMS push
- America's Sexual Health Report Card Contains Some Surprises
- Years of Excess Weight, Not One Bad Checkup, Drive Heart Disease Risk
- There Are No Good Ways To Avoid Childhood Eczema But Many Treatment Options
- More Children, Teens At Risk From E-Scooter Crashes, Study Finds
- This Treatment Can Improve Your Odds Of Surviving C. Diff Infection
- Alzheimer’s Tests May Mask Risks for Women
- RFK Jr. launching health podcast to expose ‘hypocrisy’ and ‘corruption’
- RFK Jr. launching health podcast to expose ‘hypocrisy’ and ‘corruption’
- Advocate Health improves to 4% operating margin, $4.6B bottom line across 2025
- States Face Another Challenge With Medicaid Work Rules: Staffing Shortages

- Farm Bureau Health Plans Beat the ACA on Prices With an Age-Old Tactic: Rejecting Sick People

- Avalyn plans IPO to fund phase 3 trials of inhaled versions of approved respiratory drugs
- Judge rules that HHS must face states' lawsuit over RFK Jr.'s agency overhaul, massive layoffs
- Judge rules that HHS must face states' lawsuit over RFK Jr.'s agency overhaul, massive layoffs
- Consumers' satisfaction with health plan apps improves with familiarity: JD Power
- Nurses' job satisfaction stumbles after post-pandemic gains: survey
- Amazon launches 2 new digital health partnerships for nutrition therapy, sleep care in health conditions program
- Former NFL Star Steve McMichael Diagnosed With CTE After His Death
- Steven Ubl set to depart after more than a decade as CEO of PhRMA
- Nixing prior auth, outlier hospital bills could lower health costs, Center for American Progress' policy plan says
- Shionogi nabs initial $119M award from BARDA to establish US antibiotic plant
- More Drugmakers Join TrumpRx
- Graco Recalls Infant Car Seats Over Structural Issue
- Orlando Health fleshes out Alabama footprint with another acquisition
- US adults still turn to providers for accurate health information even as AI chatbot use grows: Pew survey
- Pfizer walks away from 'underutilized' office space in South San Francisco, transitions employees to remote roles
- Biogen settles investor lawsuit over its messaging on failed Alzheimer's drug Aduhelm
- Digital health startups raked in $4B during Q1 with 12 megadeals driving investment: Rock Health
- New Cervix-On-A-Chip May Revolutionize STI Treatment
- The Flu Vaccine Can Lower Your Risk Of Heart Attack And Stroke — Even If You Wind Up Infected
- Long COVID Linked to Heart Health Risks
- Herbal Drug Kava Poses Increasing Health Threat In U.S., CDC Warns
- Preschoolers' Solitary Screen Time Could Mean Behavior Problems, Language Difficulties Later On
- Combo Heat Waves/Droughts Will Affect Billions A Year By 2100, Researchers Project
- Amgen CEO netted $24.7M pay package in ‘25 as company’s upward trajectory continued
- J&J's Tremfya retakes TV drug ad spending crown from AbbVie
- Trump’s Personnel Agency Is Asking for Federal Workers’ Medical Records

- Urgent Care Clinics Move To Fill Abortion Care Gaps in Rural Areas

- FDA Approves First Generic Farxiga (dapagliflozin) Tablets
- Reliance on EHR vendors' tech roadmap slows down AI progress, senior IT leaders say
- ¿Puedo decirle a mi médico que no quiero que use la inteligencia artificial para tomar notas?

- Remarks at the Texas Stock Exchange Event: Welcome to the Boom Belt: A Return to First Principles in Public Markets


Barak Richman, the Bartlett Professor of Law and Business Administration at Duke University posted a thought provoking opinion on Politico yesterday. Using the University of North Carolina as an example, he notes that:
One answer — albeit a distressing one — is that UNC, like many large universities, is really a hospital system with a university appendage. UNC Health has a budget that is about $2.2 billion more than the entirety of UNC’s flagship campus in Chapel Hill ($3.5 billion vs $5.5 billion). This is also true for North Carolina’s private universities that operate health systems, like Duke University, whose health system has a budget $1.1 billion larger than the remainder of the university ($4.5 billion vs $3.4 billion). Moreover, both health systems are growing faster than the rest of both campuses.These facts are important because the financial health of hospitals is highly dependent on political decisions. For example, the North Carolina General Assembly’s legislative session this year included debates over Medicaid expansion, which would infuse enormous sums of additional dollars into the state’s health sector, and “ certificate of need” rules that would govern whether current hospitals could prevent competition from new entrants. The legislature — like all other state legislatures — also routinely makes decisions on insurance eligibility, the array of services that medical professionals may offer (so called scope-of-practice rules) and the tax-exempt status of many health care facilities.
So, perhaps it is not surprising that UNC leaders prioritized legislation that enhanced the financial security of its hospital system rather than measures that would protect its Chapel Hill faculty. And perhaps it is not surprising the University of Pennsylvania, MIT and Harvard — each of which rely heavily on government, foundation and industry funding (UPenn’s health system has a budget that is more than twice the university’s) — might seek presidents who exhibit the cautious effectiveness of corporate leaders, who can assure cooperation with policymakers and compromise with ideologues, rather than visionaries who inspire resoluteness and can mount an aggressive defense against Rep Elise Stefanik (R-N.Y.).
Professor Richman's main concern is a corrosive effect on academic freedom, but a larger view would note that the managements of universities with substantial health systems will focus on their health care subsidiaries to the detriment of their educational subsidiaries.
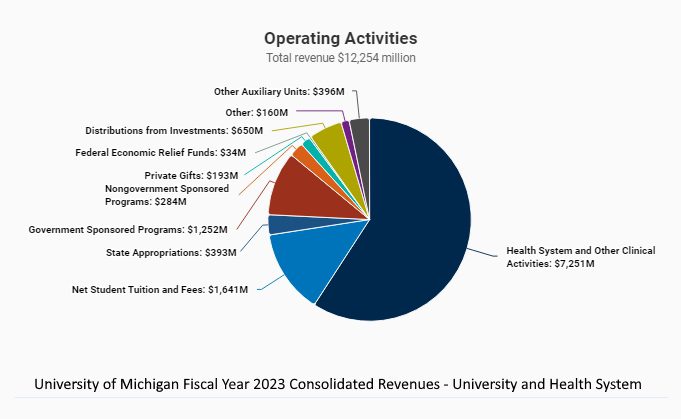
Looking at Michigan's largest university health system, we see the same effect:
And the supremacy of U of M's health care operations is growing rapidly every year:
https://2023.annualreport.umich.edu/leadership-messages/chief-financial-officers-report/
https://2022.annualreport.umich.edu/leadership-messages/chief-financial-officers-report/
{kind=link}
Barak Richman, the Bartlett Professor of Law and Business Administration at Duke University posted a thought provoking opinion on Politico yesterday. Using the University of North Carolina as an example, he notes that:
One answer — albeit a distressing one — is that UNC, like many large universities, is really a hospital system with a university appendage. UNC Health has a budget that is about $2.2 billion more than the entirety of UNC’s flagship campus in Chapel Hill ($3.5 billion vs $5.5 billion). This is also true for North Carolina’s private universities that operate health systems, like Duke University, whose health system has a budget $1.1 billion larger than the remainder of the university ($4.5 billion vs $3.4 billion). Moreover, both health systems are growing faster than the rest of both campuses.These facts are important because the financial health of hospitals is highly dependent on political decisions. For example, the North Carolina General Assembly’s legislative session this year included debates over Medicaid expansion, which would infuse enormous sums of additional dollars into the state’s health sector, and “ certificate of need” rules that would govern whether current hospitals could prevent competition from new entrants. The legislature — like all other state legislatures — also routinely makes decisions on insurance eligibility, the array of services that medical professionals may offer (so called scope-of-practice rules) and the tax-exempt status of many health care facilities.
So, perhaps it is not surprising that UNC leaders prioritized legislation that enhanced the financial security of its hospital system rather than measures that would protect its Chapel Hill faculty. And perhaps it is not surprising the University of Pennsylvania, MIT and Harvard — each of which rely heavily on government, foundation and industry funding (UPenn’s health system has a budget that is more than twice the university’s) — might seek presidents who exhibit the cautious effectiveness of corporate leaders, who can assure cooperation with policymakers and compromise with ideologues, rather than visionaries who inspire resoluteness and can mount an aggressive defense against Rep Elise Stefanik (R-N.Y.).
Professor Richman's main concern is a corrosive effect on academic freedom, but a larger view would note that the managements of universities with substantial health systems will focus on their health care subsidiaries to the detriment of their educational subsidiaries.
Looking at Michigan's largest university health system, we see the same effect:
And the supremacy of U of M's health care operations is growing rapidly every year:
https://2023.annualreport.umich.edu/leadership-messages/chief-financial-officers-report/
https://2022.annualreport.umich.edu/leadership-messages/chief-financial-officers-report/
The government of Michigan will have to soon decide whether the Board of Regents form of management dictated by Michigan's 1963 Constitution is still well suited to operating this institution.
Get MHF Insights
News and tips for your healthcare freedom.
We never spam you. One-step unsubscribe.
Sponsors
Friends of MHF




")
Kirsten DeVries
Tom & Karen Nunheimer
Steve Ahonen
Ron & Faith Bosserman
Marlin & Kathy Klumpp
Sign Up for MHF Insights to keep up on the latest in Michigan Health Policy

