- Infection prevention is an enterprise risk boards can’t delegate away

- UT Health San Antonio launches workforce program with $6.5M gift
- New York system medical chief to exit role
- Heartland Dental’s 3-year growth recap: 30+ moves
- Penn Medicine Lancaster General Health taps associate COO
- Cencora’s $10B+ physician acquisition spree: A breakdown
- Scaling DSOs: Why Integration & Liquidity Planning Matter Now

- Elizabeth Holmes’ prison sentence trimmed by 1 year
- Tennessee physician practice acquired
- HCA Florida unveils air ambulance service for rural communities
- The FTC is coming for healthcare consolidation: 10 things physicians need to know
- Adventist Health sees momentum from insourcing revenue cycle operations
- Adventist Health sees momentum from insourcing revenue cycle operations
- 19 women making moves in healthcare
- Beyond coverage: Why health systems must reframe anesthesia as an enterprise operating model
- Indiana Orthopedic Institute to open outpatient clinic
- Unlicensed dentistry cases, DSO deals, legislation & more: 10 dentistry updates in Virginia
- Missouri system debuts mobile behavioral health unit
- Yale researchers study GLP-1’s potential for SUD
- Inside Surgery Partners’ 5-year strategy pivot
- Inside Rothman Orthopaedics’ physician growth
- Texas dental school receives $6.5M to expand pediatric dental, medical programs
- Medical Clinic of Houston adds Dr. Jordan Shapiro
- North Carolina autism provider to expand therapy access
- $3M Verdict Links Social Media to Anxiety and Depression
- The worst states for physicians in the last 5 years
- West Virginia hospital to end OB delivery services
- Dr. Kevin Liu named interim GI chief at the University of Arizona
- 6 DSOs making headlines
- California hospital’s finances improve, cash position remains ‘dire’
- 1 in 5 metro markets face inpatient monopoly: 7 notes
- Minnesota system faces uncertainty amid Medicare delays
- Ohio county approves behavioral health crisis center plan
- The White House Delays CDC Pick
- 4 health systems outsourcing RCM functions
- Mayo Clinic receives $75M gift for logistics hub project
- New COVID 'Cicada' Variant Is Spreading — What Experts Want You To Know
- EP ablation in the ASC: Opportunity meets operational reality
- Family Caregivers Provide $1 Trillion In Annual Labor, AARP Says
- Want A Bootlicking Yes Man? Ask An AI Chatbot For Advice, Study Warns
- Specially Coated Implants Better For Breast Cancer Patients, Study Finds
- At-Home Chemotherapy Is Safe, Feasible, Pilot Study Indicates
- ‘Health Doesn’t Need to Be Ludacris’: Bayer signs rapper-actor to multivitamin campaign
- Rocket plots measured trajectory for new gene therapy Kresladi after clearance to launch from FDA
- New Cholesterol Guidelines: What Patients and Caregivers Need to Know
- What You Do While Sitting Could Predict Dementia Risk
- Healthy Lab Results May Mask Future Risks for Kids with Obesity
- Give and Take: Federal Rural Health Funding Could Trigger Service Cuts

- Trump Team Claims Successes Against ACA Fraud While Pushing for More Controls

- Fierce Pharma Asia—Takeda’s $1.3B reorg; India’s GLP-1 floodgates; Gilead’s $2.2B buy of a China NewCo
- Where are you with EUDAMED?

- Where are you with EUDAMED?
- HL7 Launches Real‑Time Medical Device Interoperability Accelerator
- HL7 Launches Real‑Time Medical Device Interoperability Accelerator
- Two GA Tech ATDC Startups — Nephrodite and OrthoPreserve — Secure FDA Breakthrough Device Designation
- Two GA Tech ATDC Startups — Nephrodite and OrthoPreserve — Secure FDA Breakthrough Device Designation
- Artificial Intelligence: ROI, not Clinical Autonomy, Leads Operational Workflows
- Artificial Intelligence: ROI, not Clinical Autonomy, Leads Operational Workflows
- Medtronic and Merit Medical Systems distribution agreement for new, ViaVerte basivertebral nerve ablation system
- Medtronic and Merit Medical Systems distribution agreement for new, ViaVerte basivertebral nerve ablation system
- Breakthrough Device Designation for Noah Labs Vox Heart Failure Detection Device
- Breakthrough Device Designation for Noah Labs Vox Heart Failure Detection Device
- Why private practice dentistry needs a better model
- CareQuest Innovation Partners, Kno2 collab on medical-dental data integration
- The hospitals, health systems cutting jobs in 2026
- Nonprofit highlights rural opioid care strategies
- The 7 things on the table in the Mount Sinai-Anthem negotiations
- Vitana Pediatric & Orthodontic Partners adds Florida practice
- Providence narrows operating loss to $486M in 2025
- What the Health? From KFF Health News: A Headless CDC

- Rhode Island oral surgeon launches Congressional campaign
- 20 behavioral health leaders challenge industry assumptions
- Recordati confirms it's weighing CVC Capital buyout offer of $12.6B
- 3 California behavioral health centers to close amid funding shifts
- Indiana bars autism therapy provider from Medicaid billing: Wall Street Journal
- 6 dental practice openings to know
- UnitedHealth shareholder sues over proposal to include details on integration in annual proxy
- APRNs, PAs account for most antipsychotic prescriptions for Medicare Part D: Study
- SCAN taps biopharma, CMS vet Aman Bhandari as its first chief AI officer
- Infosys to acquire Optimum Healthcare IT in $465M deal
- Oklahoma House passes bill expanding scope of dental assistants
- California behavioral health agency to close 2 centers
- DOJ alleges NewYork-Presbyterian forces payers into anticompetitive 'all-or-nothing' contracts
- FDA Warns Biotech Firm Over Cancer Drug Anktiva Claims
- Bees and Hummingbirds May Be Consuming Small Amounts of Alcohol
- Two States Sue Cord Blood Company Over Misleading Claims
- New WHO Guidance Aims To Speed Tuberculosis Testing
- As questions swirl around ATTR competition, Alnylam plots path to market leadership for Amvuttra
- Trump admin delays nomination for new CDC director past deadline
- Outspoken ACIP member steps down amid vaccine panel uncertainty: reports
- Egg-based drugmaker Neion Bio emerges from stealth to cook up multi-product biosimilar collab
- Genentech walks the walk in lupus as sponsor of annual awareness and fundraising event
- Study Reveals How Many Americans Consider Using a Gun
- Massive Study Finds Stress and Grief Don’t Cause Cancer
- Ultra-Processed Foods Harm Fertility In Both Men And Women, Studies Reveal
- Small Daily Habits Can Add Up To Better Heart Health
- Ritalin Might Protect ADHD Kids' Long-Term Mental Health, Study Finds
- Can You Drink Enough Fluids To Prevent Kidney Stones? Maybe Not, New Study Says
- Clasp, loan-linked hiring tool for employers, clinches $20M to expand amid federal loan caps
- Taking a GLP-1? Doctors Say Not To Forget About Movement and Mental Health

- OpenEvidence rolls out AI medical coding feature
- CDC’s Acting Chief Promises a Return to Stability in a Tumultuous Moment

- Remarks at the Financial Stability Oversight Council Meeting
- RWJF: Between 5M and 10M people could lose Medicaid coverage in 2028 under work requirements
- New therapy animal program aims to support 100K patients, providers
- Pulse check on Lilly's GLP-1 fortunes
- Gen Z nurses prioritize schedule flexibility, need more manager interactions to avoid turnover
- How pharma marketers can capitalize on HCPs’ AI, social media and streaming habits
- Federal Officials Investigate States That Require Abortion Coverage
- Corcept's lead drug bounces back from FDA snub with different approval as Lifyorli in ovarian cancer
- Ionis slashes Tryngolza's price tag by 93% ahead of anticipated label expansion
- FDA approves Denali's Hunter syndrome drug, handing rare disease community a win
- Baby Walkers Sold on Amazon Recalled Over Fall Risk
- Want To Protect Your Brain? Science Says Exercise
- HelloFresh Pizza Recall Issued in 10 States Over Metal Risk
- Clinical Trials Have Too Much Data…That’s the Problem.

- Clinical Trials Have Too Much Data…That’s the Problem.
- CMS reveals new Medicaid model that supports coordination for children with complex needs
- Novartis sued by breast cancer patient over branded drug websites’ data-sharing practices
- Takeda targets $1.3B in cost savings in further restructuring
- Biogen pays $20M upfront to tap into Alteogen's subQ delivery tech
- 'Universal Donor' Blood Supplies Dangerously Low, Study Warns
- Why Stepping Outside May Help You Eat Better
- U.S. Medicine, Science Facing An Online Misinformation Siege, Poll Concludes
- Childhood Obesity Undercuts The American Dream For Some, Study Says
- Inclusive High Schools Benefit All Students, Not Just LGBTQ Teens
- Parental Loss Due to Drugs, Violence Raises Child Death Risk by 2,000%
- As Boehringer touts US launches, board chairman worries EU is 'falling further behind'
- The evolving state of exome and genome sequencing
- An Arm and a Leg: Steep Health Care Costs Steer Americans to Tough Decisions

- Demoralized CDC Workforce Reels From Year of Firings, Funding Cuts, and a Shooting

- Qualified Health locks in $125M in fresh funding to scale enterprise AI at health systems
- Misery Loves [Investment] Company?: Remarks at the 2026 Investment Company Institute Investment Management Conference
- Study: Nearly 1 in 5 pediatric hospital deaths involve sepsis
- As expansions come online, CDMO Hovione aims to meet industry's 'dual supply and sourcing' zeal: exec
- Opening Remarks at the Digital Asset Summit 2026
- CVS Caremark, FTC reach settlement in insulin pricing case
- UCB unveils plan to build $2B biologics plant near its US headquarters in Atlanta
- PeaceHealth sued over plans to tap out-of-state staffer ApolloMD for Oregon EDs
- New Lyme Disease Vaccine Shows Strong Results in Trial
- TrumpRx Adds Diabetes, COPD Drugs at Steep Discounts
- Highmark reports $175M net loss for 2025 as financial headwinds batter health plan
- Listen to the Latest ‘KFF Health News Minute’

- Abivax hires commercial chief from Takeda to infuse Entyvio expertise into IBD launch prep
- ImmunityBio hit with FDA warning letter over Anktiva promotions in TV ad, podcast episode
- Alcohol Prep Pads Recalled Over Bacteria Risk, Cardinal Health Says
- Fewer patients traveled for abortions in 2025 as telehealth care increased, report finds
- Cologuard campaign reunites ‘Full House’ stars to give ‘The Talk’ about colon cancer screening
- Karyopharm, looking to jump-start Xpovio, reports mixed results in myelofibrosis
- Study Warns Fluoride Bans May Raise Tooth Decay in Children


The Paragon Health Institute has been running a series challenging the OBBBA Medicaid myths. Here are their most recent challenges to the top 10 myths being promulgated to politically damage the OBBBA:
https://paragoninstitute.org/private-health/myth-the-obbb-will-result-in-large-coverage-losses/
Myth: The OBBB will result in large coverage losses
Key Facts
- There are roughly 12 million ineligible enrollees in Medicaid expansion and the Obamacare exchanges—the result of the Biden administration’s enrollment-at-any-cost strategy. Eligibility review requirements in the OBBB will help ensure that only those legally eligible for coverage will receive it.
- One-quarter of the estimated number of ineligible recipients comes from Democrats’ intentional sunset of Biden’s COVID credits—the enhanced Affordable Care Act (ACA) subsidies in their 2022 reconciliation bill, which is unrelated to the OBBB.
- Nearly one-third of the estimated number comes from the Congressional Budget Office’s estimate of people who will not meet the OBBB’s work and community-engagement requirement. More than 80% of the American people support requirements for able-bodied, working-age adults to work to receive a welfare benefit. These requirements can be met by 80 hours of work, job training, education, or volunteer service each month.
- The claims about lost coverage depend on the CBO, which has an extremely poor track record when estimating the impact of legislation on health coverage. For example, CBO was off by a factor of more than 10 with its estimate of coverage losses associated with eliminating the ACA’s individual mandate penalty.
Background
The Biden administration pursued an enrollment-at-any-cost strategy that led to massive numbers of ineligible people being enrolled, many of whom use no health care services and are unaware of their enrollment. The Biden administration permitted unchecked fraud rings to grow that misled applicants and enrolled them without their knowledge. In 2025, 45 percent of all exchange enrollees took no action and were automatically re-enrolled in fully or near-fully subsidized plans. More than 6.4 million people are enrolled in fully subsidized exchange plans who are not eligible. States also have massive incentives to improperly enroll people in the ACA’s Medicaid expansion because they get seven times more federal funding for every $1 of spending on expansion enrollees than on traditional enrollees. Medicaid’s improper payment rate exceeds 25 percent, largely because states abandoned proper eligibility rules. We estimate that there are at least 6 million ineligible Medicaid expansion enrollees in 2025.
The OBBB ultimately will help the poor and vulnerable by focusing Medicaid and the ACA on them and their needs, instead of driving hundreds of billions of taxpayer dollars into the pockets of insurers, big hospitals, and fraudsters. Verifying eligibility and reducing fraud doesn’t mean that those who lose coverage have no options. Millions will have access to subsidized exchange plans or employer coverage. And able-bodied, working-age adults should have to work or show meaningfully productive activity to be eligible for a government welfare program. Not only is it the right principle, but this policy benefits these adults by encouraging them to work, build skills, and engage with their community.
https://paragoninstitute.org/medicaid/myth-the-obbb-medicaid-reforms-are-unpopular/
Myth: The OBBB Medicaid reforms are unpopular.
Key Facts
Americans support the core Medicaid reforms in the OBBB. In a poll of 1,000 registered voters, commissioned by Paragon, Americans overwhelmingly support:
- Removing Ineligible Enrollees: Paragon polling shows 64 percent of Americans believe the government has a responsibility to taxpayers as well as legitimate Medicaid recipients to ensure that only those who are eligible can enroll in Medicaid.
- Work Requirements for Able-Bodied Adults: More than 80 percent of Americans support requiring able-bodied, working-age adults to engage in 80 hours of work, job training, education, or volunteering monthly to maintain Medicaid eligibility.
- Medicaid Payment Parity with Medicare: 83 percent of Americans agree that Medicaid should not pay providers more than Medicare for the same services, as this inflates costs and harms access for seniors.
- Limiting Financing Gimmicks Like Provider Taxes: 57 percent of Americans believe provider taxes are a way that states take advantage of federal taxpayers to cushion their budgets and cater to health care special interests.
Background
The OBBB reforms Medicaid to restore program integrity and focus the program on the truly vulnerable—low-income children, pregnant women, the elderly, and the disabled. Polls organized by the OBBB opponents typically mislead voters by implying reforms harm these groups. Advocates of the bloated status quo often cite polls, like those from the Kaiser Family Foundation, claiming Americans oppose Medicaid reforms. Yet these polls fail to ask balanced questions about the specific policies in the OBBB.
The OBBB targets waste, fraud, and abuse in the program and the key reforms like work requirements and increased eligibility reviews are targeted only at the able-bodied, working-age adult ACA expansion enrollees.
The Biden administration’s enrollment-at-any-cost strategy led to millions of ineligible enrollees, including 6 million in Medicaid expansion, with an improper payment rate exceeding 25 percent. States exacerbate waste by using financing gimmicks like provider taxes to then make inflated payments to insurers and hospitals. President Obama proposed limits on provider taxes, which were very similar to the provisions in the OBBB. His vice president at the time, Joe Biden, referred to provider taxes as a “scam” that should be eliminated.
https://paragoninstitute.org/medicaid/myth-the-obbb-cuts-medicaid/
Myth: The OBBB cuts Medicaid.
Key Facts
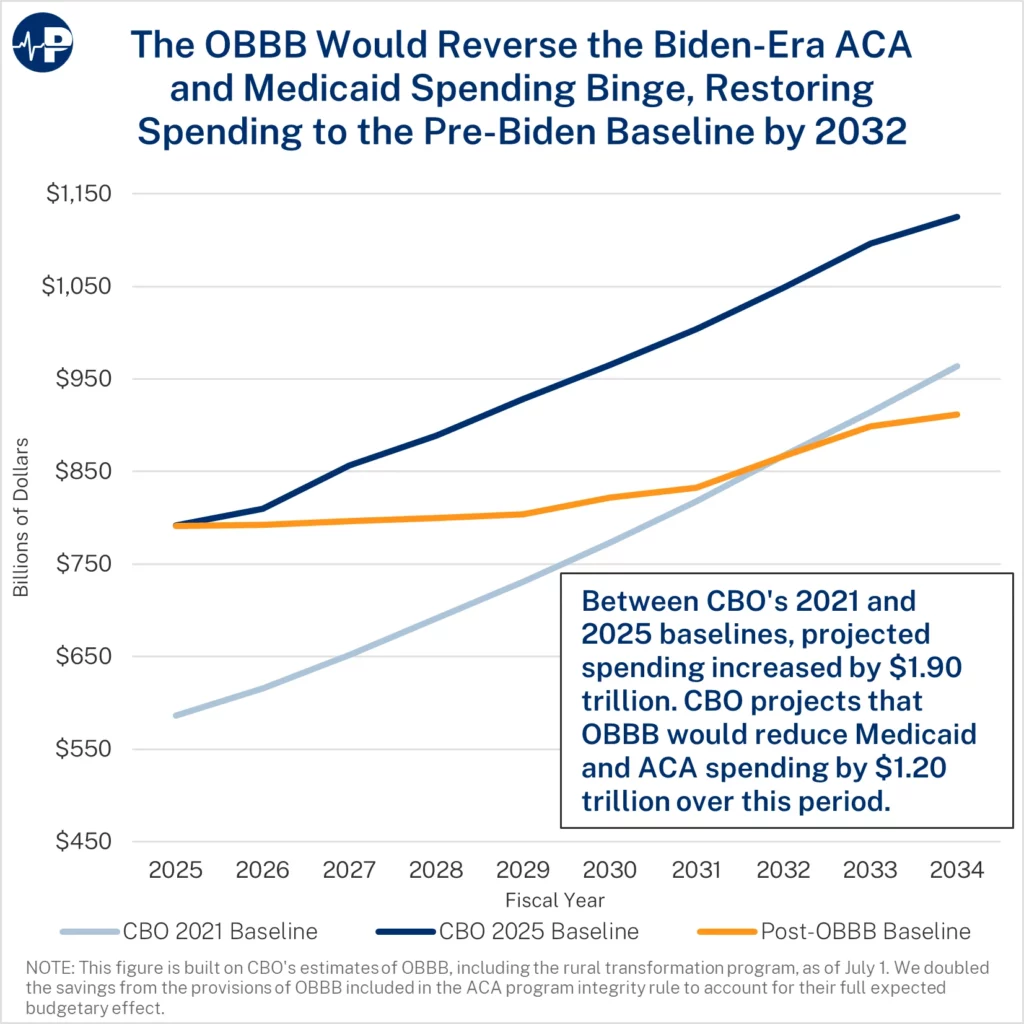
- There are no cuts to Medicaid. OBBB slows spending growth, putting the program on a more sustainable path.
- For four years, the Biden administration pursued an enrollment-at-any-cost agenda, which dramatically increased federal subsidies to health insurers and big hospital systems.
- As a result, the federal baseline for Medicaid and Affordable Care Act (ACA) subsidies increased by $1.9 trillion over the next decade between the 2021 and 2025 baselines.
- OBBB addresses the Medicaid money-laundering machine, promotes work and personal responsibility in Medicaid, reduces the number of improper enrollees in Medicaid and the ACA exchanges, and reverses costly Biden regulations.
Background
There are more than 12 million improper enrollees in Medicaid expansion and the ACA exchanges combined in 2025. This problem stems from dramatically higher subsidies and curtailed eligibility verifications. Fraud rings misled exchange applicants about free perks, coached them to misstate income, and profited from commissions—while insurers reaped windfalls. Improper exchange enrollment will cost the government nearly $30 billion this year and improper federal Medicaid payments equal $1.1 trillion over the past decade.
Myth: The OBBB’s Medicaid provisions will force nursing homes to close
Key Facts
- Key provisions of the OBBB that reduce the growth of federal Medicaid spending will not affect nursing homes or their residents. These provisions—community-engagement requirements and more frequent eligibility reviews—are focused only on the able-bodied, working-age adults added to Medicaid under Obamacare.
- By rescinding the Biden Administration Nursing Home Minimum Staffing rule, nursing homes will face fewer costs to comply with government mandates, will gain flexibility and cost savings, be able to hire at more appropriate staff levels, and will be less likely to close— particularly in rural areas, where nursing homes were most at risk.
- The legislation also excludes nursing homes from the OBBB’s provider tax phasedown that occurs in Medicaid expansion states since nursing homes serve seniors, a traditional Medicaid group. This exemption should ease concerns from OBBB critics focused on short-term provider tax revenue losses.
- Federal policy, due to Obamacare, creates large incentives for states to direct Medicaid resources away from seniors and people with disabilities and toward able-bodied, working-age adults. States currently receive an average of seven times more in federal funding for every $1 they spend on expansion adults versus every $1 they spend on traditional enrollees.
Background
The OBBB effectively rescinds the Biden administration’s nationwide mandate on nursing home staffing. This Biden mandate, which was finalized in 2024, would have cost more than $40 billion over 10 years, imposed rigid minimum staffing ratios regardless of facility size or patient needs, and presented a major threat to rural and lower-margin homes. Those homes would have likely reduced care for their vulnerable residents. A 2023 survey showed 94 percent of nursing homes already faced staffing shortages. By overturning the rule, the OBBB lifts costly mandates and allows facilities to adjust staffing based on patient needs and local workforce conditions—helping avoid declines in care quality and potential closures.
Nursing homes also suffer under Obamacare’s funding formula, which gives states $9 in federal funds for every $1 spent on able-bodied, working-age adults, but only $1.33 for every $1 spent on seniors or people with disabilities. This disparity skews resources toward expansion adults at the expense of traditional enrollees. In states that adopted Obamacare’s expansion, OBBB adopts an Obama administration proposal to reduce Medicaid money laundering schemes by limiting the amount that states can raise through provider taxes to generate federal matching dollars. Provider taxes are particularly harmful when states funnel the money through expansion enrollees since they receive a much higher federal match. Nursing homes are specifically exempted from the provider tax phasedown because they serve traditional enrollees, not expansion enrollees.
By refocusing Medicaid on the truly vulnerable, the OBBB helps to protect seniors and individuals with disabilities. The OBBB reforms will result in lower state and federal Medicaid spending on able-bodied, working-age adults, preserving resources for those who truly need Medicaid, such as nursing home residents and people with disabilities.
https://paragoninstitute.org/medicaid/correcting-the-record-on-community-engagement-requirements/
Correcting the Record on Community Engagement Requirements
Myth: The OBBB community-engagement requirements will kick millions of workers off Medicaid.
Fact: The Congressional Budget Office estimates that nearly five million able-bodied, working-age adults will not meet the work and community-engagement requirements. Unfortunately, a large and growing number of able-bodied, working-age individuals, particularly men, have chosen not to work or look for work. Time-use surveys suggest that many Medicaid expansion enrollees are spending large amounts of time watching television, playing video games, and sleeping ten or more hours a day. The Centers for Medicaid and Medicare Services is committed to working with states to ensure that eligible enrollees who satisfy the community-engagement requirements remain covered in Medicaid.
Myth: Children and the disabled will be kicked off Medicaid due to the work requirements.
Fact: The community-engagement requirements only apply to able-bodied, working-age adults who do not have children age 13 or younger and who are enrolled under Obamacare’s expansion. In households with children age 14 or older, eligible children will still be enrolled in the program even if their parent do not meet the community-engagement requirements.
Myth: People will not be able to find jobs and will lose Medicaid eligibility as a result.
Fact: The legislation allows for exemptions from the community-engagement requirements in areas with high unemployment. Additionally, there are numerous avenues for individuals to satisfy the 80-hour-a-month community-engagement requirements. This includes volunteering, work training, attending school, or any combination of these activities for a total of 80 hours a month.
Myth: Two-thirds of able-bodied, working-age adults on Medicaid already work, so we do not need these requirements.
Fact: A significant number of the 20 million able-bodied working-age adults that have Medicaid through the ACA expansion do not work or meet other community-engagement criteria. Allowing able-bodied, working-age adults to receive benefits without satisfying community-engagement requirements is unfair to those able-bodied, working-age adults on Medicaid who work as well as the most vulnerable who most need the program.
Myth: OBBB just punishes the poor.
Fact: President Clinton, when signing the 1996 welfare to work law, clearly articulated that a system that traps people on welfare is what punishes the poor.
“Nearly 30 years ago, Robert Kennedy said, ‘‘Work is the meaning of what this country is all about. We need it as individuals, we need to sense it in our fellow citizens, and we need it as a society and as a people.’’ He was right then, and it’s right now. From now on, our Nation’s answer to this great social challenge will no longer be a never-ending cycle of welfare, it will be the dignity, the power, and the ethic of work. Today we are taking an historic chance to make welfare what it was meant to be: a second chance, not a way of life.”
The vast majority of Americans agree with these remarks today. More than two of three Americans believe that “Medicaid should be a temporary safety net, not a long-term entitlement for those who are able to work. Encouraging this population to work would improve their personal situation and help get them off Medicaid, saving money that could be directed toward those who need it most—children, seniors, and people with disabilities.”
Working leads to better health. The Robert Wood Johnson Foundation has found unemployment leads to worse health outcomes and increases in stress related conditions such as strokes, heart attacks and arthritis. It also found that unemployment increases the incidence of depression.
Myth: Seasonal workers will not be able to comply because their work schedules vary.
Fact: Seasonal workers will meet the requirements if their average monthly income over the past six months is at least equal to the minimum wage for 80 hours of work per month.
Myth: As previous attempts at work requirements show, they are impossible to administer.
Fact: The federal government has had work requirements for federal welfare programs since 1996, when President Clinton signed the Personal Responsibility and Work Opportunity Reconciliation Act, otherwise known as welfare reform.
Previous state-level attempts to implement work requirements, which are often cited by critics of the policy, were done on an ad hoc basis through state waiver requests. Supporters of the ever-expanding welfare state fought against work requirements and sued the state, making implementation more difficult. Now, instead of relying on one-off waivers, the Centers for Medicare and Medicaid Services will provide states with implementation guidance, technical assistance, and model programs.
States will also be eligible to receive implementation grants to build the necessary systems. This assistance was not available to those states that previously attempted to implement work requirements through a waiver.
Finally, technology has progressed significantly since 2018. Information tools and platforms to administer these requirements have advanced, and what was once seen as futuristic—like Artificial Intelligence—is now a promising frontier for every sector of the U.S. economy.
Background
The One Big Beautiful Act institutes community-engagement requirements for able-bodied, working-age adults who do not have children younger than 14 and who are enrolled under Obamacare’s expansion. These requirements can be satisfied through working 80 hours a month. Alternatively, the requirements can be satisfied through volunteering, job training, or going to school.
The OBBB provides exemptions from the requirements to ensure they are directed at individuals who can satisfy them. These exemptions include:
- Parents, guardians, and family caregivers of disabled individuals or children age 13 or younger,
- Medically frail individuals or those with special medical needs,
- Individuals participating in drug addiction or alcoholic treatment and rehabilitation programs, and
- Individuals that satisfy the Supplemental Nutrition Assistance Program work requirements.
Myth: States will not be able to cope with the limits on Medicaid money-laundering mechanisms.
Key facts
- The One Big Beautiful Bill (OBBB) Medicaid reforms would incentivize states to prioritize caring for the needy, not using the federal government as a cash cow.
- States now pay the lowest share of Medicaid expenses in history—driven by Medicaid money laundering and Obamacare.
- Under the Biden administration’s policies, Medicaid money laundering exploded with provider taxes inflating Medicaid payment rates well above Medicare rates.
- The OBBB adopts an Obama-era proposal to phase down provider taxes from 6.0 percent to 3.5 percent starting in 2028 in Medicaid expansion states—an annual 0.5 percent decrease. The bill also freezes provider taxes, so states can’t increase this funding scam after July 4, 2025.
- The OBBB implements stricter rules on provider taxes to curb egregious state abuses, such as a managed care tax that California used to draw down $10 billion in federal funds without spending any of its own money. The next year, California expanded Medicaid to unauthorized immigrants.
- The Biden administration issued a rule that states could make Medicaid payments through insurers up to average commercial rates, which average 2.5 times Medicare rates. The OBBB ensures that Medicaid rates, through health insurers, are capped at or just above Medicare rates. More than 80 percent of voters support capping Medicaid rates at Medicare levels.
Background
Leaders of both parties have expressed concern about provider tax schemes. In 2011, then Vice President Biden called them a “scam.” President Obama’s 2013 budget first proposed reforms to phase down the provider tax safe harbor from 6.0 percent to 3.5 percent. The safe harbor is effectively the amount that states can tax providers and leverage that revenue to obtain federal matching funds, which are then used to make large payments to the taxed providers. In many instances, states keep some of the extra federal funding to use on unrelated programs. The OBBB also helps CMS better ensure that taxes on providers are broad-based and uniform. These requirements prevent states from disproportionately taxing entities that receive the benefit of higher Medicaid payments, a sure sign that the tax is meant for money laundering rather than a legitimate revenue source.
In part due to states’ increased use of Medicaid money-laundering, the federal government now covers 75 percent of Medicaid spending—far above the historic 60 percent share. As states now contribute less than their historic share of Medicaid, they have less incentive to care about results. Instead, they use Medicaid as a federal cash cow for their state coffers. This dynamic reduces states’ incentives to run their Medicaid programs efficiently.
The OBBB limits state proposals not submitted by the date of enactment to Medicare rates in Medicaid expansion states (and 110 percent of Medicare rates in non-expansion states) and would gradually phase down payments above Medicare rates until they comply. This mirrors the existing cap for Medicaid rates when paid through fee for service. Medicaid paying much more than Medicare threatens seniors’ access to care by leading providers to prioritize Medicaid over Medicare.
https://paragoninstitute.org/medicaid/myth-rural-hospitals-will-close-because-of-the-obbb/
Myth: Rural hospitals will close because of the OBBB.
Key Facts
- The OBBB’s reforms to limit waste, fraud, abuse, and corporate welfare in Medicaid—projected to save nearly $900 billion over the next decade—enabled new funding to support rural health care providers and ensure access to core medical services in rural areas.
- The OBBB provides $10 billion in annual funding over the next five years to improve and transform rural health care access, including support for existing rural facilities.
- States increasingly use financial schemes resembling money-laundering, which disproportionately benefit large, urban, and well-connected hospital systems.
- A recent Paragon study found no evidence that provider taxes—the most common Medicaid money laundering scheme—help boost employment in rural hospitals. Our findings suggest provider taxes may harm rural hospitals. In 2023, states with hospital provider taxes had markedly lower population-adjusted employment among rural hospitals than states without these taxes.
- Rural hospitals already benefit from at least nine federal subsidy programs. For example, many of these facilities qualify as Critical Access Hospitals (CAHs), allowing them to garner additional payments through Medicare.
Background
In 2024, only $10 billion, about 5 percent, of $214 billion in total inpatient Medicaid spending went to rural hospitals, with most of the remainder supporting urban facilities. There are numerous government programs aimed at shoring up rural providers, including Critical Access Hospitals (CAHs), Medicare-Dependent Hospitals, and Low-Volume Hospitals.
The OBBB takes critical steps to limit financing schemes that direct government funding toward large, corporate hospital systems. These reforms, plus community engagement requirements, more frequent eligibility reviews for Obamacare expansion enrollees, and rolling back costly Biden regulatory actions, are projected to save nearly $900 billion over the next decade. As a result of enacting needed Medicaid reforms and reversing Biden’s spending binge, Congress created $10 billion in annual grants for states to target funding to support rural health care providers, ensure access to core medical services in rural areas, and transform rural health care delivery.
The widespread use of Medicaid money laundering tactics to lavish higher government payments on big hospitals and insurers has simply not benefitted rural providers. For example, provider taxes—mechanisms used by states to draw down federal tax dollars—have disproportionately benefitted large, well-connected hospital systems. Universal Health Services, for example, netted $1 billion from these schemes last year. Additionally, linking Medicaid payment rates to average commercial rates contributes to rising commercial hospital prices.
A recent empirical analysis from Paragon found no evidence that provider taxes are supporting employment in rural hospital systems—and may even harm them. Employment levels help gauge whether facilities are offering new or expanded services, growing their capacity, and contributing to the local economy. Rural hospital employment in states implementing a hospital provider tax dramatically declines compared to states that never imposed such financing schemes and worsens with time.
https://paragoninstitute.org/medicaid/myth-the-obbb-largely-repeals-the-affordable-care-act/
Myth: The OBBB largely repeals the Affordable Care Act.
Key Facts
- The One Big Beautiful Bill (OBBB) focuses on reversing many of the Biden administration’s enrollment-at-any-cost policies that led to 6.4 million improper exchange enrollees and $27 billion in improper spending in 2025. This enrollment fraud largely benefited health insurers and unscrupulous brokers.
- Although certain structures of the Affordable Care Act (ACA) have increased health insurance and health care costs, the OBBB does not modify any of the ACA’s insurance rules, the subsidies for ACA exchange plans, or the 90 percent state reimbursement for the Medicaid expansion population.
- The OBBB will undo the Biden administration’s cost-inflating Special Enrollment Period (SEP) based on income, which exacerbated fraud and raised premiums by encouraging people to wait until they were sick to enroll. The Obama administration never authorized an income-based SEP.
- The OBBB will also require annual eligibility checks. These provisions mirror requirements proposed or implemented by the Obama administration. President Biden undercut commonsense eligibility checks, which contributed to a surge in enrollment fraud. The Centers for Medicare & Medicaid Services (CMS) previously estimated that submitting similar information would take just 45 to 60 minutes.
- When President Trump first came to office, he strengthened the ACA exchanges by expanding eligibility verification and reducing gaming of the system. As a result, premiums grew more slowly year-over-year under the Trump administration than under the Obama administration.
- By requiring annual eligibility checks and increasing repayment for excess advanced subsidies, the OBBB restores wise governance and accountability in the ACA exchanges. The OBBB also limits exchange subsidies to U.S. citizens and legal residents.
Background
The OBBB will require annual eligibility verification for people to receive subsidies before they enroll. Both Presidents Obama and Trump proposed or implemented such eligibility checks, which President Biden undercut.
The OBBB also gets rid of the Biden administration’s SEP that allows low-income people to sign up at any point in the year. The Biden-era SEP flies in the face of the ACA’s language, which only allows the Secretary of Health and Human Services to create SEPs, if they are similar to Medicare’s allowable SEPs, such as getting married, having a child, or losing your job. This SEP also increases premiums by encouraging people to wait until they get sick to sign up for insurance. CMS estimates the SEP for households earning 100 to 150 percent of the federal poverty line increased premiums from 0.5 to 3.6 percent a year. The SEP also made it easier for fraudsters to sign people up for the ACA without their permission.
Because the enhanced ACA subsidies resulted in fully subsidized plans for those claiming between 100 and 150 percent of the federal poverty line, many rogue brokers signed up millions of people for ACA plans, often without their knowledge. In the first three months of 2024, this SEP alone generated over 50,000 complaints of improper enrollment and 40,000 unauthorized plan switches.
Myth: The OBBB will harm the most vulnerable Medicaid enrollees.
Key Facts
- The OBBB will improve access to care for the most vulnerable Medicaid enrollees—low-income children, pregnant women, the elderly, and people with disabilities—by refocusing the program on them.
- Since 2013, Medicaid rolls have swelled under the Affordable Care Act. More than 20 million able-bodied, working-age adults to Medicaid. These new enrollees, who now account for about 25 percent of Medicaid enrollees nationwide, have put additional strain on the health care system and diverted resources away from vulnerable Medicaid enrollees
- Excessive federal reimbursements for Medicaid expansion enrollees and lax federal rules have fueled rampant enrollment fraud. A recent Paragon analysis estimated that about 6.6 million enrollees classified in the expansion group likely earn too much to qualify for coverage. Yet, prior to the OBBB, states had virtually no incentive to combat ineligible enrollment, making it more difficult for traditional enrollees to obtain care.
- The OBBB implements long-overdue reforms to restore program integrity to Medicaid and ensure that care is delivered to traditional Medicaid enrollees. The OBBB puts in place:
- More frequent eligibility checks and community-engagement requirements for able-bodied adults covered through the ACA expansion.
- Cost-sharing requirements for able-bodied adults covered under the ACA expansion to protect taxpayers from wasteful health care spending.
- Enhanced penalties for states with high Medicaid improper payment rates, specifically for errors stemming from ineligible enrollment.
- Restrictions on illegal immigrants accessing Medicaid benefits.
Background
Ensuring access to timely, high-quality care for patients on Medicaid has been a long-standing challenge. Prior to the ACA, studies showed that Medicaid patients had inferior access to care and worse health outcomes than comparable individuals with private coverage. Yet instead of heeding these warning signs and taking steps to improve the program for the most vulnerable Americans, the federal government has recklessly expanded enrollment to new able-bodied adult populations. Predictably, as new enrollees compete for a limited pool of providers, access to care for traditional Medicaid enrollees has eroded.
Numerous academic studies have found evidence that enrolling able-bodied adults undermined access to care for vulnerable enrollees. A 2022 study from the Mercatus Center found that per-capita Medicaid spending on children grew much more slowly in Medicaid expansion states than in non-expansion states from 2013 to 2019, implying that needy children likely faced greater barriers to care. A meta-analysis found that prior to the ACA, Medicaid patients were only half as likely to obtain a doctor’s appointment as the privately insured. Post-ACA, Medicaid patients’ chances declined to less than one-third relative to the privately insured. A 2021 analysis of emergency department data reported that Medicaid expansion caused a 10 percent increase in the amount of time spent waiting to be seen, as well as a 15 percent increase in the proportion of patients who left without seeing a provider.
https://paragoninstitute.org/medicaid/myth-there-is-little-waste-fraud-and-abuse-in-medicaid/
Myth: There is little waste, fraud, abuse in Medicaid.
Key Facts
- Proponents of the bloated, bureaucratic status quo claim that there is little waste, fraud, and abuse in the nearly $1 trillion Medicaid program.
- Paragon research estimates nearly $1.2 trillion in improper federal Medicaid payments—a 25 percent improper payment rate—over the past decade.
- The OBBB contains significant Medicaid reforms—addressing Medicaid money-laundering schemes and requiring able-bodied, working-age adults to perform community-engagement requirements.
- In addition, OBBB further addresses the rampant Medicaid waste, fraud, and abuse in a myriad of ways, including more frequent eligibility reviews of able-bodied, working-age ACA expansion enrollees, requiring states to reduce the improper payment rates, no longer paying health plans for individuals enrolled in multiple states, and making sure taxpayers are not paying for Medicaid coverage for the deceased.
- The OBBB institutes systems to prevent individuals from being enrolled in Medicaid in multiple states at one time.
- A recent Wall Street Journal report indicated that insurers received $4.3 billion for Medicaid enrollees simultaneously enrolled in multiple states from 2019 to 2021.
- On July 17, the Centers for Medicare and Medicaid Services (CMS) announced it found 1.2 million people enrolled in multiple state Medicaid programs and 1.6 million people doubly covered by Medicaid and a subsidized exchange plan. CMS estimates that its corrective actions will save $14 billion annually—a massive victory for taxpayers.
- The OBBB requires states to check the Death Master File quarterly to remove deceased Medicaid enrollees and deceased providers.
Background
Under current law, states are supposed to be penalized for improper payment rates above three percent. But this policy has never been enforced; states can receive waivers, permitting waste to continue unabated. The OBBB would limit the ability of the HHS Secretary to waive commonsense, good governance requirements to combat improper payments.
Under the OBBB, there will now be an enforceable budget-neutrality requirement for Medicaid demonstration projects or waivers. States run much of their programs through waivers. Theoretically, this allows states to tailor their programs to the unique needs of their enrollees and test new approaches for the delivery of Medicaid services.
Demonstration projects are supposed to be budget neutral (i.e., not result in more federal spending than would occur absent the waiver). However, lax enforcement and inflated baseline projections often result in demonstrations imposing steep costs on the federal government. The OBBB requires CMS to certify the demonstration’s budget-neutrality requirements for a waiver to be granted.

Get MHF Insights
News and tips for your healthcare freedom.
We never spam you. One-step unsubscribe.
Sponsors
Friends of MHF




")
Kirsten DeVries
Tom & Karen Nunheimer
Steve Ahonen
Ron & Faith Bosserman
Marlin & Kathy Klumpp
Sign Up for MHF Insights to keep up on the latest in Michigan Health Policy

