







- Facing Funding Losses, States Call Out Big Businesses With Employees on Medicaid

- Physician pay drops, ACOs gain under CMS’ 2027 proposal: 8 things to know

- This psychiatric hospital CEO wants to retire the term ‘co-occurring’
- Physician assistant median pay hits $135K: State-by-state breakdown
- AI in the healthcare workforce: 4 notes
- CHOP increased naloxone co-prescribing from 3% to 84%: Study
- HCA now expects up to $1.2B hit from ACA headwinds
- Teladoc named preferred virtual care provider for NBA players union
- Automation Paid Off—So Why Are Denials Still Rising?
- 3 Russians indicted in $62M cybercrime scheme that hit hospitals
- CMS floats 1.68% cut to physician fee schedule, 7 other things to know
- Orthopedic robotics company lands up to $65M in growth capital
- 25 health systems dropping Medicare Advantage plans | 2026
- HCA names divisional CIO
- Minnesota system names interim CEO
- The America medical education system is not behaving as a normal market
- New York awards $6.3M for mental health clubhouses
- Smile Partners USA continues de novo strategy with new practice
- 988 crisis line tops 23M contacts since launch: 5 things to know
- Bipartisan Senate bill targets ASC Medicare reimbursement gap
- Outpatient care to grow 3x faster than inpatient: Report
- Average gross billings for owner dentists surpassed $1M in 2025
- CMS proposes major Medicare reforms to shift physician pay, phase out MIPS and expand ACO participation
- Specialty Dental Brands selects Videa as its AI platform
- States with the most, fewer psychologists per capita
- Oregon State Hospital named in wrongful death lawsuit
- Mobile care DSO Smile America Partners acquired by investment firm
- With FDA approval for its breast cancer blockbuster hopeful, Celcuity could ‘belong in the hands’ of a Big Pharma
- The specialties winning ASC procedure access — and losing on payment
- Anthropic pushes deeper into healthcare with Optum tie-up, UST integration
- FTC, CVS unveil settlement in ongoing insulin pricing case
- Are ASCs still the right investment? 3 orthopedic surgeons make the case
- What physicians miss when selling their ASC
- Why ASCs may not need a $1.5M spine robot
- North Carolina eye surgeon asks for reversal in CON trial
- HHS promises its final rule barring pediatric gender care providers from Medicare is still coming
- FDA issues psychedelic drug clinical trial guidance: 8 things to know
- AMA interoperability initiative brings structured clinical terminology to CPT codes
- Director's Note on What to Expect at the 2026 Partnerships with Sites Summit
- Rising Tide Dental Partners expands network by 22%, appoints COO
- Lettuce Suspected In Growing Multistate Cyclospora Outbreak
- Startup Sonata launches preventive healthcare membership, linking clinical decisions with AI
- Why Are Family Doctors Leaving The Workforce? Retirement, Burnout Creating A U.S. Primary Care 'Brain Drain'
- HCA Healthcare now expects ACA exchange impacts to exceed $1B in 2026
- Huyabio scores with Opdivo combo in 'milestone' skin cancer trial
- Unruly Patients Are Stressing ER Staff, Undermining Care
- Pain Patients Should Taper Opioids At Their Own Pace, Study Suggests
- Heatwaves Raise Hospital Admissions For Mental Health Woes
- U.S. Gun Suicides Hit Record High, Even As Firearm Deaths Decline Overall
- AstraZeneca pays up to $1.5B for EGFR lung cancer drug Zegfrovy from its spinoff Dizal
- Worried About Your Aging Parents? Welcome To The Caregiving Club
- Lawmakers Look To Make Abortion Shield Laws Less Dependent on Who’s Governor

- Knee Pain? Ragged Cartilage? Research Suggests Surgery’s Not the Best Answer

- Real Chemistry builds body of AI healthcare commercialization tools with Anatomi launch
- Inside agency view: Havas SO on authenticity, connection and pushing back against the ‘sea of sameness’
- Why policy gaps threaten behavioral health coverage
- Specialty dentist pay vs. cost of living by state
- HHS, VA sign agreement to advance psychedelic therapy
- What the de novo boom means for DSOs
- Pearl vs. Videa vs. Overjet: what 3 AI giants have accomplished in 2026
- 8 dental Medicaid updates for dentists to know
- What DSO success looks like in the new age of dentistry
- Cellares' recent automated cell therapy wins have 'opened the biotech floodgates'
- Insulet, Calm join forces for diabetes care offerings with ‘Mind in Range’ wellness tools
- Hospital M&A stays hot in Q2 as health systems position for the future
- 13 behavioral health services, facility closures | 2026
- Cottage Health Expands Partnership with hellocare.ai Following Successful Pilot to Deploy AI Assisted Virtual Care and Patient Safety Platform Enterprise Wide
- North Carolina budget allocates millions for first-ever Rural Emergency Hospital reopening
- Payer-backed ad campaign urges lawmakers to reject NSA enforcement bill
- What Is An Aortic Dissection? The Condition That Killed Sen. Lindsey Graham
- Insurers set to pay out $759M in 2026 MLR rebates: KFF
- Weight-Loss Drugs Help, But Exercise Is Still The Key To A Healthier Heart
- FDA's latest onshoring move homes in on streamlined facility registration, foreign plant scrutiny
- Germany pushes through healthcare reform package despite pharma's drug discount resistance
- GSK to seek FDA approval for Jemperli in small but high-profile cancer use after phase 2 win
- Smartphones Can Increase Seniors' Risk Of Depression
- Pro Soccer Players Show Signs Of Shrinking Brains
- Adderall Misuse Falls Sharply Among Young Adults, Study Finds
- New KFF Poll Reveals Who Is Most Likely To Endorse Vaccine Myths
- A New Option For Long-Term Care Costs
- As GOP Cries Fraud, Newsom Backs Medicaid Spending on Housing and Food

- Lupin recalls more than 2.5M prescription eye drop bottles, citing possible contamination
- Digital health funding hits $7.4B in 2026 as AI investment reshapes the market
- Journalists Discuss Raw-Milk Marketing, Extreme Heat, Opioid Settlement Spending

- Doctors want wearable data but healthcare isn't ready for it, AMA survey finds
- Feds push back HIPAA security rule overhaul to July 2027
- Katie Couric's Memory Loss Scare Puts Rare Brain Condition In Spotlight
- Mild COVID Can Lead To Long-Term Hidden Eye Problems
- Star Padcev-Keytruda combo expands bladder cancer reach with FDA approval, pressuring AstraZeneca
- ACO REACH participants generated nearly $1B in 2024 savings: CMS
- Young people living with PKU take the mic in BioMarin podcast series, TikTok push
- Apollo inks €3B equity deal for stake in Bayer's contraceptives business
- Op-ed: Tackling affordability is a shared responsibility. Here's what hospitals are doing
- Pearl Health banks $110M in fresh funding to build out tech and AI for Medicare providers
- FDA rejects Hengrui, Elevar’s PD-1 liver cancer combo for a 3rd time
- LGBTQ+ People Less Likely To Be Screened For Some Common Cancers
- Smartphone App Uses Voice To Predict Asthma, COPD Flare-Ups
- Seniors Know How Sharp They Are At Any Given Time, Study Finds
- Patients Face A Thicket of Red Tape Trying To Maintain Consistent Health Coverage
- AI Can Detect Previously Invisible MS Scars In The Brain
- A New Option for Long-Term Care Costs

- They Harvest the Nation’s Food, but a New Rule May Strip Them of Health Insurance

- Sanofi snags FDA thumbs up for Sarclisa as 1st cancer drug delivered by on-body injector
- Fierce Pharma Asia—More AZ China deals; Kailera, Hengrui’s oral GLP-1 data; Scrutiny of Chinese trials
- J&J’s Tremfya retakes ad spending throne in June as Haleon tops pharma’s World Cup airings
- Former Mayo Clinic research director sues system over alleged retaliation for raising AI practice concerns
- A $10B deal, China trial scrutiny and highlights from ADA 2026
- Remarks at the Society for Corporate Governance Conference
- GLP-1 Use Hits Record High As Medicare Opens Access To Weight-Loss Drugs
- Beyond Benchmarks: Why Trust Must Be Built into Clinical AI Infrastructure
- Foundation Fights Medical Errors That Claim 200,000 U.S. Lives A Year
- Weekly Rundown: Surgical Safety Technologies rebrands to Aimbient; UC San Diego launches applied health intelligence institute
- New, Highly Accurate Brush Test Can Detect Mouth Cancer Within An Hour
- Innovative Hip Replacement Cuts Post-Surgery Risk Of Dislocation By 70%
- Global Study Finds Kids Worldwide Skipping Fruits And Vegetables
- Affordable Care Act Insurers Want More Premium Increases As Enrollment Sags
- My Search for a Psychiatric Bed in an Overburdened Health System

- How Lee Health Turned Language Access into a Strategic Clinical Asset
- Decision readiness is the next AI advantage
- E. Coli Outbreak Prompts Recall Of Frozen Blueberries At Publix
- Drinking Coffee May Lower Your Risk of Liver Disease
- Zimmer Biomet to Hire 500 in India as New Bengaluru Technology Centre Drives AI and MedTech Innovation
- AdaptHealth Investigates Data Breach After Social Engineering Attack, Possible Link to ShinyHunters Emerges
- Rumination Plays Key Role In Caregiver Stress, Study Says
- U.S. Teens Underestimate Risks Of Fentanyl Use, Survey Finds
- Men More Likely To Be Diagnosed With Advanced Cancer
- Copay Assistance Is Meant To Defray Patient Drug Costs. Some Insurers Keep It Instead.
- Training Program Could Ward Off Injuries Among Soccer Girls
- Affordable Care Act Insurers Want More Premium Increases as Enrollment Sags

- Patients Face a Thicket of Red Tape Trying To Maintain Consistent Health Coverage

- Accountability Is Key to Medicaid's Home Care Future
- Clinical Success Is No Longer One Number
- Thousands of Medicare Beneficiaries Thought Their Drug Plan Was Free. Then They Lost It.
- Michigan, Other States See Unusual Spike In Parasite That Causes 'Explosive' Diarrhea
- Statement on the 2026 Regulatory Agenda
- 9 of the Top 10 Pharma Manufacturers Partner with Redi Health to Lead the Next-Generation Patient Experience
- GLP-1 'Secret Shopper' Study Finds Gaps in Online Prescribing
- Applying Agentic AI to Healthcare Delivery: The Key to True Transformation

- From Compliance to Clinical Action: Fixing the Broken Loop in Post-Market Surveillance

- Fatty Liver Boosts Odds Of More Deadly Colon Cancer, Study Says
- Weight Loss Surgery Increases Risk Of Alcoholism, Study Says
- IV Vitamin C Might Boost Recuperation Among Trauma Patients
- SCAN Health Plan, Alignment Healthcare sue to challenge CMS' MA star ratings recalculations
- Regulatory tracker: Eisai, Biogen scoop up subQ Leqembi starter dose nod
- Remarks at the Economic Club of New York
- Is Your Organization Ready to Govern AI in Regulatory Affairs?

- CMS Proposes TAVR Medicare Coverage is Potential Boost for Edwards Lifesciences
- Remarks to the US-CEE Connection: Transatlantic Challenges in Law, Business & Policy
- Statement Regarding Minimum Pricing Increments and Access Fee Caps
- Statement at the SEC Open Meeting on the Trade-Through Rule and Locked and Crossed Markets Provisions of Regulation NMS
Michigan healthcare freedom community forum

The Paragon Health Institute has been running a series challenging the OBBBA Medicaid myths. Here are their most recent challenges to the top 10 myths being promulgated to politically damage the OBBBA:
https://paragoninstitute.org/private-health/myth-the-obbb-will-result-in-large-coverage-losses/
Myth: The OBBB will result in large coverage losses
Key Facts
- There are roughly 12 million ineligible enrollees in Medicaid expansion and the Obamacare exchanges—the result of the Biden administration’s enrollment-at-any-cost strategy. Eligibility review requirements in the OBBB will help ensure that only those legally eligible for coverage will receive it.
- One-quarter of the estimated number of ineligible recipients comes from Democrats’ intentional sunset of Biden’s COVID credits—the enhanced Affordable Care Act (ACA) subsidies in their 2022 reconciliation bill, which is unrelated to the OBBB.
- Nearly one-third of the estimated number comes from the Congressional Budget Office’s estimate of people who will not meet the OBBB’s work and community-engagement requirement. More than 80% of the American people support requirements for able-bodied, working-age adults to work to receive a welfare benefit. These requirements can be met by 80 hours of work, job training, education, or volunteer service each month.
- The claims about lost coverage depend on the CBO, which has an extremely poor track record when estimating the impact of legislation on health coverage. For example, CBO was off by a factor of more than 10 with its estimate of coverage losses associated with eliminating the ACA’s individual mandate penalty.
Background
The Biden administration pursued an enrollment-at-any-cost strategy that led to massive numbers of ineligible people being enrolled, many of whom use no health care services and are unaware of their enrollment. The Biden administration permitted unchecked fraud rings to grow that misled applicants and enrolled them without their knowledge. In 2025, 45 percent of all exchange enrollees took no action and were automatically re-enrolled in fully or near-fully subsidized plans. More than 6.4 million people are enrolled in fully subsidized exchange plans who are not eligible. States also have massive incentives to improperly enroll people in the ACA’s Medicaid expansion because they get seven times more federal funding for every $1 of spending on expansion enrollees than on traditional enrollees. Medicaid’s improper payment rate exceeds 25 percent, largely because states abandoned proper eligibility rules. We estimate that there are at least 6 million ineligible Medicaid expansion enrollees in 2025.
The OBBB ultimately will help the poor and vulnerable by focusing Medicaid and the ACA on them and their needs, instead of driving hundreds of billions of taxpayer dollars into the pockets of insurers, big hospitals, and fraudsters. Verifying eligibility and reducing fraud doesn’t mean that those who lose coverage have no options. Millions will have access to subsidized exchange plans or employer coverage. And able-bodied, working-age adults should have to work or show meaningfully productive activity to be eligible for a government welfare program. Not only is it the right principle, but this policy benefits these adults by encouraging them to work, build skills, and engage with their community.
https://paragoninstitute.org/medicaid/myth-the-obbb-medicaid-reforms-are-unpopular/
Myth: The OBBB Medicaid reforms are unpopular.
Key Facts
Americans support the core Medicaid reforms in the OBBB. In a poll of 1,000 registered voters, commissioned by Paragon, Americans overwhelmingly support:
- Removing Ineligible Enrollees: Paragon polling shows 64 percent of Americans believe the government has a responsibility to taxpayers as well as legitimate Medicaid recipients to ensure that only those who are eligible can enroll in Medicaid.
- Work Requirements for Able-Bodied Adults: More than 80 percent of Americans support requiring able-bodied, working-age adults to engage in 80 hours of work, job training, education, or volunteering monthly to maintain Medicaid eligibility.
- Medicaid Payment Parity with Medicare: 83 percent of Americans agree that Medicaid should not pay providers more than Medicare for the same services, as this inflates costs and harms access for seniors.
- Limiting Financing Gimmicks Like Provider Taxes: 57 percent of Americans believe provider taxes are a way that states take advantage of federal taxpayers to cushion their budgets and cater to health care special interests.
Background
The OBBB reforms Medicaid to restore program integrity and focus the program on the truly vulnerable—low-income children, pregnant women, the elderly, and the disabled. Polls organized by the OBBB opponents typically mislead voters by implying reforms harm these groups. Advocates of the bloated status quo often cite polls, like those from the Kaiser Family Foundation, claiming Americans oppose Medicaid reforms. Yet these polls fail to ask balanced questions about the specific policies in the OBBB.
The OBBB targets waste, fraud, and abuse in the program and the key reforms like work requirements and increased eligibility reviews are targeted only at the able-bodied, working-age adult ACA expansion enrollees.
The Biden administration’s enrollment-at-any-cost strategy led to millions of ineligible enrollees, including 6 million in Medicaid expansion, with an improper payment rate exceeding 25 percent. States exacerbate waste by using financing gimmicks like provider taxes to then make inflated payments to insurers and hospitals. President Obama proposed limits on provider taxes, which were very similar to the provisions in the OBBB. His vice president at the time, Joe Biden, referred to provider taxes as a “scam” that should be eliminated.
https://paragoninstitute.org/medicaid/myth-the-obbb-cuts-medicaid/
Myth: The OBBB cuts Medicaid.
Key Facts
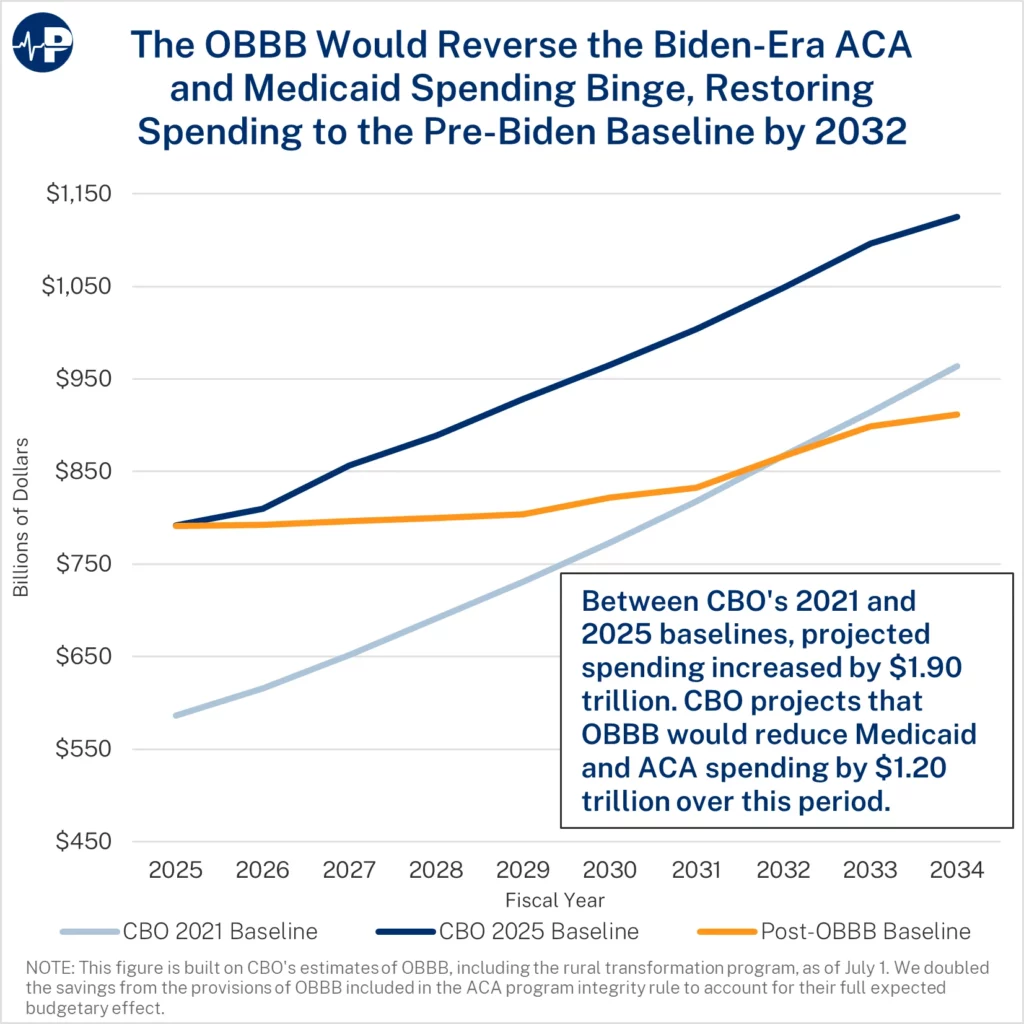
- There are no cuts to Medicaid. OBBB slows spending growth, putting the program on a more sustainable path.
- For four years, the Biden administration pursued an enrollment-at-any-cost agenda, which dramatically increased federal subsidies to health insurers and big hospital systems.
- As a result, the federal baseline for Medicaid and Affordable Care Act (ACA) subsidies increased by $1.9 trillion over the next decade between the 2021 and 2025 baselines.
- OBBB addresses the Medicaid money-laundering machine, promotes work and personal responsibility in Medicaid, reduces the number of improper enrollees in Medicaid and the ACA exchanges, and reverses costly Biden regulations.
Background
There are more than 12 million improper enrollees in Medicaid expansion and the ACA exchanges combined in 2025. This problem stems from dramatically higher subsidies and curtailed eligibility verifications. Fraud rings misled exchange applicants about free perks, coached them to misstate income, and profited from commissions—while insurers reaped windfalls. Improper exchange enrollment will cost the government nearly $30 billion this year and improper federal Medicaid payments equal $1.1 trillion over the past decade.
Myth: The OBBB’s Medicaid provisions will force nursing homes to close
Key Facts
- Key provisions of the OBBB that reduce the growth of federal Medicaid spending will not affect nursing homes or their residents. These provisions—community-engagement requirements and more frequent eligibility reviews—are focused only on the able-bodied, working-age adults added to Medicaid under Obamacare.
- By rescinding the Biden Administration Nursing Home Minimum Staffing rule, nursing homes will face fewer costs to comply with government mandates, will gain flexibility and cost savings, be able to hire at more appropriate staff levels, and will be less likely to close— particularly in rural areas, where nursing homes were most at risk.
- The legislation also excludes nursing homes from the OBBB’s provider tax phasedown that occurs in Medicaid expansion states since nursing homes serve seniors, a traditional Medicaid group. This exemption should ease concerns from OBBB critics focused on short-term provider tax revenue losses.
- Federal policy, due to Obamacare, creates large incentives for states to direct Medicaid resources away from seniors and people with disabilities and toward able-bodied, working-age adults. States currently receive an average of seven times more in federal funding for every $1 they spend on expansion adults versus every $1 they spend on traditional enrollees.
Background
The OBBB effectively rescinds the Biden administration’s nationwide mandate on nursing home staffing. This Biden mandate, which was finalized in 2024, would have cost more than $40 billion over 10 years, imposed rigid minimum staffing ratios regardless of facility size or patient needs, and presented a major threat to rural and lower-margin homes. Those homes would have likely reduced care for their vulnerable residents. A 2023 survey showed 94 percent of nursing homes already faced staffing shortages. By overturning the rule, the OBBB lifts costly mandates and allows facilities to adjust staffing based on patient needs and local workforce conditions—helping avoid declines in care quality and potential closures.
Nursing homes also suffer under Obamacare’s funding formula, which gives states $9 in federal funds for every $1 spent on able-bodied, working-age adults, but only $1.33 for every $1 spent on seniors or people with disabilities. This disparity skews resources toward expansion adults at the expense of traditional enrollees. In states that adopted Obamacare’s expansion, OBBB adopts an Obama administration proposal to reduce Medicaid money laundering schemes by limiting the amount that states can raise through provider taxes to generate federal matching dollars. Provider taxes are particularly harmful when states funnel the money through expansion enrollees since they receive a much higher federal match. Nursing homes are specifically exempted from the provider tax phasedown because they serve traditional enrollees, not expansion enrollees.
By refocusing Medicaid on the truly vulnerable, the OBBB helps to protect seniors and individuals with disabilities. The OBBB reforms will result in lower state and federal Medicaid spending on able-bodied, working-age adults, preserving resources for those who truly need Medicaid, such as nursing home residents and people with disabilities.
https://paragoninstitute.org/medicaid/correcting-the-record-on-community-engagement-requirements/
Correcting the Record on Community Engagement Requirements
Myth: The OBBB community-engagement requirements will kick millions of workers off Medicaid.
Fact: The Congressional Budget Office estimates that nearly five million able-bodied, working-age adults will not meet the work and community-engagement requirements. Unfortunately, a large and growing number of able-bodied, working-age individuals, particularly men, have chosen not to work or look for work. Time-use surveys suggest that many Medicaid expansion enrollees are spending large amounts of time watching television, playing video games, and sleeping ten or more hours a day. The Centers for Medicaid and Medicare Services is committed to working with states to ensure that eligible enrollees who satisfy the community-engagement requirements remain covered in Medicaid.
Myth: Children and the disabled will be kicked off Medicaid due to the work requirements.
Fact: The community-engagement requirements only apply to able-bodied, working-age adults who do not have children age 13 or younger and who are enrolled under Obamacare’s expansion. In households with children age 14 or older, eligible children will still be enrolled in the program even if their parent do not meet the community-engagement requirements.
Myth: People will not be able to find jobs and will lose Medicaid eligibility as a result.
Fact: The legislation allows for exemptions from the community-engagement requirements in areas with high unemployment. Additionally, there are numerous avenues for individuals to satisfy the 80-hour-a-month community-engagement requirements. This includes volunteering, work training, attending school, or any combination of these activities for a total of 80 hours a month.
Myth: Two-thirds of able-bodied, working-age adults on Medicaid already work, so we do not need these requirements.
Fact: A significant number of the 20 million able-bodied working-age adults that have Medicaid through the ACA expansion do not work or meet other community-engagement criteria. Allowing able-bodied, working-age adults to receive benefits without satisfying community-engagement requirements is unfair to those able-bodied, working-age adults on Medicaid who work as well as the most vulnerable who most need the program.
Myth: OBBB just punishes the poor.
Fact: President Clinton, when signing the 1996 welfare to work law, clearly articulated that a system that traps people on welfare is what punishes the poor.
“Nearly 30 years ago, Robert Kennedy said, ‘‘Work is the meaning of what this country is all about. We need it as individuals, we need to sense it in our fellow citizens, and we need it as a society and as a people.’’ He was right then, and it’s right now. From now on, our Nation’s answer to this great social challenge will no longer be a never-ending cycle of welfare, it will be the dignity, the power, and the ethic of work. Today we are taking an historic chance to make welfare what it was meant to be: a second chance, not a way of life.”
The vast majority of Americans agree with these remarks today. More than two of three Americans believe that “Medicaid should be a temporary safety net, not a long-term entitlement for those who are able to work. Encouraging this population to work would improve their personal situation and help get them off Medicaid, saving money that could be directed toward those who need it most—children, seniors, and people with disabilities.”
Working leads to better health. The Robert Wood Johnson Foundation has found unemployment leads to worse health outcomes and increases in stress related conditions such as strokes, heart attacks and arthritis. It also found that unemployment increases the incidence of depression.
Myth: Seasonal workers will not be able to comply because their work schedules vary.
Fact: Seasonal workers will meet the requirements if their average monthly income over the past six months is at least equal to the minimum wage for 80 hours of work per month.
Myth: As previous attempts at work requirements show, they are impossible to administer.
Fact: The federal government has had work requirements for federal welfare programs since 1996, when President Clinton signed the Personal Responsibility and Work Opportunity Reconciliation Act, otherwise known as welfare reform.
Previous state-level attempts to implement work requirements, which are often cited by critics of the policy, were done on an ad hoc basis through state waiver requests. Supporters of the ever-expanding welfare state fought against work requirements and sued the state, making implementation more difficult. Now, instead of relying on one-off waivers, the Centers for Medicare and Medicaid Services will provide states with implementation guidance, technical assistance, and model programs.
States will also be eligible to receive implementation grants to build the necessary systems. This assistance was not available to those states that previously attempted to implement work requirements through a waiver.
Finally, technology has progressed significantly since 2018. Information tools and platforms to administer these requirements have advanced, and what was once seen as futuristic—like Artificial Intelligence—is now a promising frontier for every sector of the U.S. economy.
Background
The One Big Beautiful Act institutes community-engagement requirements for able-bodied, working-age adults who do not have children younger than 14 and who are enrolled under Obamacare’s expansion. These requirements can be satisfied through working 80 hours a month. Alternatively, the requirements can be satisfied through volunteering, job training, or going to school.
The OBBB provides exemptions from the requirements to ensure they are directed at individuals who can satisfy them. These exemptions include:
- Parents, guardians, and family caregivers of disabled individuals or children age 13 or younger,
- Medically frail individuals or those with special medical needs,
- Individuals participating in drug addiction or alcoholic treatment and rehabilitation programs, and
- Individuals that satisfy the Supplemental Nutrition Assistance Program work requirements.
Myth: States will not be able to cope with the limits on Medicaid money-laundering mechanisms.
Key facts
- The One Big Beautiful Bill (OBBB) Medicaid reforms would incentivize states to prioritize caring for the needy, not using the federal government as a cash cow.
- States now pay the lowest share of Medicaid expenses in history—driven by Medicaid money laundering and Obamacare.
- Under the Biden administration’s policies, Medicaid money laundering exploded with provider taxes inflating Medicaid payment rates well above Medicare rates.
- The OBBB adopts an Obama-era proposal to phase down provider taxes from 6.0 percent to 3.5 percent starting in 2028 in Medicaid expansion states—an annual 0.5 percent decrease. The bill also freezes provider taxes, so states can’t increase this funding scam after July 4, 2025.
- The OBBB implements stricter rules on provider taxes to curb egregious state abuses, such as a managed care tax that California used to draw down $10 billion in federal funds without spending any of its own money. The next year, California expanded Medicaid to unauthorized immigrants.
- The Biden administration issued a rule that states could make Medicaid payments through insurers up to average commercial rates, which average 2.5 times Medicare rates. The OBBB ensures that Medicaid rates, through health insurers, are capped at or just above Medicare rates. More than 80 percent of voters support capping Medicaid rates at Medicare levels.
Background
Leaders of both parties have expressed concern about provider tax schemes. In 2011, then Vice President Biden called them a “scam.” President Obama’s 2013 budget first proposed reforms to phase down the provider tax safe harbor from 6.0 percent to 3.5 percent. The safe harbor is effectively the amount that states can tax providers and leverage that revenue to obtain federal matching funds, which are then used to make large payments to the taxed providers. In many instances, states keep some of the extra federal funding to use on unrelated programs. The OBBB also helps CMS better ensure that taxes on providers are broad-based and uniform. These requirements prevent states from disproportionately taxing entities that receive the benefit of higher Medicaid payments, a sure sign that the tax is meant for money laundering rather than a legitimate revenue source.
In part due to states’ increased use of Medicaid money-laundering, the federal government now covers 75 percent of Medicaid spending—far above the historic 60 percent share. As states now contribute less than their historic share of Medicaid, they have less incentive to care about results. Instead, they use Medicaid as a federal cash cow for their state coffers. This dynamic reduces states’ incentives to run their Medicaid programs efficiently.
The OBBB limits state proposals not submitted by the date of enactment to Medicare rates in Medicaid expansion states (and 110 percent of Medicare rates in non-expansion states) and would gradually phase down payments above Medicare rates until they comply. This mirrors the existing cap for Medicaid rates when paid through fee for service. Medicaid paying much more than Medicare threatens seniors’ access to care by leading providers to prioritize Medicaid over Medicare.
https://paragoninstitute.org/medicaid/myth-rural-hospitals-will-close-because-of-the-obbb/
Myth: Rural hospitals will close because of the OBBB.
Key Facts
- The OBBB’s reforms to limit waste, fraud, abuse, and corporate welfare in Medicaid—projected to save nearly $900 billion over the next decade—enabled new funding to support rural health care providers and ensure access to core medical services in rural areas.
- The OBBB provides $10 billion in annual funding over the next five years to improve and transform rural health care access, including support for existing rural facilities.
- States increasingly use financial schemes resembling money-laundering, which disproportionately benefit large, urban, and well-connected hospital systems.
- A recent Paragon study found no evidence that provider taxes—the most common Medicaid money laundering scheme—help boost employment in rural hospitals. Our findings suggest provider taxes may harm rural hospitals. In 2023, states with hospital provider taxes had markedly lower population-adjusted employment among rural hospitals than states without these taxes.
- Rural hospitals already benefit from at least nine federal subsidy programs. For example, many of these facilities qualify as Critical Access Hospitals (CAHs), allowing them to garner additional payments through Medicare.
Background
In 2024, only $10 billion, about 5 percent, of $214 billion in total inpatient Medicaid spending went to rural hospitals, with most of the remainder supporting urban facilities. There are numerous government programs aimed at shoring up rural providers, including Critical Access Hospitals (CAHs), Medicare-Dependent Hospitals, and Low-Volume Hospitals.
The OBBB takes critical steps to limit financing schemes that direct government funding toward large, corporate hospital systems. These reforms, plus community engagement requirements, more frequent eligibility reviews for Obamacare expansion enrollees, and rolling back costly Biden regulatory actions, are projected to save nearly $900 billion over the next decade. As a result of enacting needed Medicaid reforms and reversing Biden’s spending binge, Congress created $10 billion in annual grants for states to target funding to support rural health care providers, ensure access to core medical services in rural areas, and transform rural health care delivery.
The widespread use of Medicaid money laundering tactics to lavish higher government payments on big hospitals and insurers has simply not benefitted rural providers. For example, provider taxes—mechanisms used by states to draw down federal tax dollars—have disproportionately benefitted large, well-connected hospital systems. Universal Health Services, for example, netted $1 billion from these schemes last year. Additionally, linking Medicaid payment rates to average commercial rates contributes to rising commercial hospital prices.
A recent empirical analysis from Paragon found no evidence that provider taxes are supporting employment in rural hospital systems—and may even harm them. Employment levels help gauge whether facilities are offering new or expanded services, growing their capacity, and contributing to the local economy. Rural hospital employment in states implementing a hospital provider tax dramatically declines compared to states that never imposed such financing schemes and worsens with time.
https://paragoninstitute.org/medicaid/myth-the-obbb-largely-repeals-the-affordable-care-act/
Myth: The OBBB largely repeals the Affordable Care Act.
Key Facts
- The One Big Beautiful Bill (OBBB) focuses on reversing many of the Biden administration’s enrollment-at-any-cost policies that led to 6.4 million improper exchange enrollees and $27 billion in improper spending in 2025. This enrollment fraud largely benefited health insurers and unscrupulous brokers.
- Although certain structures of the Affordable Care Act (ACA) have increased health insurance and health care costs, the OBBB does not modify any of the ACA’s insurance rules, the subsidies for ACA exchange plans, or the 90 percent state reimbursement for the Medicaid expansion population.
- The OBBB will undo the Biden administration’s cost-inflating Special Enrollment Period (SEP) based on income, which exacerbated fraud and raised premiums by encouraging people to wait until they were sick to enroll. The Obama administration never authorized an income-based SEP.
- The OBBB will also require annual eligibility checks. These provisions mirror requirements proposed or implemented by the Obama administration. President Biden undercut commonsense eligibility checks, which contributed to a surge in enrollment fraud. The Centers for Medicare & Medicaid Services (CMS) previously estimated that submitting similar information would take just 45 to 60 minutes.
- When President Trump first came to office, he strengthened the ACA exchanges by expanding eligibility verification and reducing gaming of the system. As a result, premiums grew more slowly year-over-year under the Trump administration than under the Obama administration.
- By requiring annual eligibility checks and increasing repayment for excess advanced subsidies, the OBBB restores wise governance and accountability in the ACA exchanges. The OBBB also limits exchange subsidies to U.S. citizens and legal residents.
Background
The OBBB will require annual eligibility verification for people to receive subsidies before they enroll. Both Presidents Obama and Trump proposed or implemented such eligibility checks, which President Biden undercut.
The OBBB also gets rid of the Biden administration’s SEP that allows low-income people to sign up at any point in the year. The Biden-era SEP flies in the face of the ACA’s language, which only allows the Secretary of Health and Human Services to create SEPs, if they are similar to Medicare’s allowable SEPs, such as getting married, having a child, or losing your job. This SEP also increases premiums by encouraging people to wait until they get sick to sign up for insurance. CMS estimates the SEP for households earning 100 to 150 percent of the federal poverty line increased premiums from 0.5 to 3.6 percent a year. The SEP also made it easier for fraudsters to sign people up for the ACA without their permission.
Because the enhanced ACA subsidies resulted in fully subsidized plans for those claiming between 100 and 150 percent of the federal poverty line, many rogue brokers signed up millions of people for ACA plans, often without their knowledge. In the first three months of 2024, this SEP alone generated over 50,000 complaints of improper enrollment and 40,000 unauthorized plan switches.
Myth: The OBBB will harm the most vulnerable Medicaid enrollees.
Key Facts
- The OBBB will improve access to care for the most vulnerable Medicaid enrollees—low-income children, pregnant women, the elderly, and people with disabilities—by refocusing the program on them.
- Since 2013, Medicaid rolls have swelled under the Affordable Care Act. More than 20 million able-bodied, working-age adults to Medicaid. These new enrollees, who now account for about 25 percent of Medicaid enrollees nationwide, have put additional strain on the health care system and diverted resources away from vulnerable Medicaid enrollees
- Excessive federal reimbursements for Medicaid expansion enrollees and lax federal rules have fueled rampant enrollment fraud. A recent Paragon analysis estimated that about 6.6 million enrollees classified in the expansion group likely earn too much to qualify for coverage. Yet, prior to the OBBB, states had virtually no incentive to combat ineligible enrollment, making it more difficult for traditional enrollees to obtain care.
- The OBBB implements long-overdue reforms to restore program integrity to Medicaid and ensure that care is delivered to traditional Medicaid enrollees. The OBBB puts in place:
- More frequent eligibility checks and community-engagement requirements for able-bodied adults covered through the ACA expansion.
- Cost-sharing requirements for able-bodied adults covered under the ACA expansion to protect taxpayers from wasteful health care spending.
- Enhanced penalties for states with high Medicaid improper payment rates, specifically for errors stemming from ineligible enrollment.
- Restrictions on illegal immigrants accessing Medicaid benefits.
Background
Ensuring access to timely, high-quality care for patients on Medicaid has been a long-standing challenge. Prior to the ACA, studies showed that Medicaid patients had inferior access to care and worse health outcomes than comparable individuals with private coverage. Yet instead of heeding these warning signs and taking steps to improve the program for the most vulnerable Americans, the federal government has recklessly expanded enrollment to new able-bodied adult populations. Predictably, as new enrollees compete for a limited pool of providers, access to care for traditional Medicaid enrollees has eroded.
Numerous academic studies have found evidence that enrolling able-bodied adults undermined access to care for vulnerable enrollees. A 2022 study from the Mercatus Center found that per-capita Medicaid spending on children grew much more slowly in Medicaid expansion states than in non-expansion states from 2013 to 2019, implying that needy children likely faced greater barriers to care. A meta-analysis found that prior to the ACA, Medicaid patients were only half as likely to obtain a doctor’s appointment as the privately insured. Post-ACA, Medicaid patients’ chances declined to less than one-third relative to the privately insured. A 2021 analysis of emergency department data reported that Medicaid expansion caused a 10 percent increase in the amount of time spent waiting to be seen, as well as a 15 percent increase in the proportion of patients who left without seeing a provider.
https://paragoninstitute.org/medicaid/myth-there-is-little-waste-fraud-and-abuse-in-medicaid/
Myth: There is little waste, fraud, abuse in Medicaid.
Key Facts
- Proponents of the bloated, bureaucratic status quo claim that there is little waste, fraud, and abuse in the nearly $1 trillion Medicaid program.
- Paragon research estimates nearly $1.2 trillion in improper federal Medicaid payments—a 25 percent improper payment rate—over the past decade.
- The OBBB contains significant Medicaid reforms—addressing Medicaid money-laundering schemes and requiring able-bodied, working-age adults to perform community-engagement requirements.
- In addition, OBBB further addresses the rampant Medicaid waste, fraud, and abuse in a myriad of ways, including more frequent eligibility reviews of able-bodied, working-age ACA expansion enrollees, requiring states to reduce the improper payment rates, no longer paying health plans for individuals enrolled in multiple states, and making sure taxpayers are not paying for Medicaid coverage for the deceased.
- The OBBB institutes systems to prevent individuals from being enrolled in Medicaid in multiple states at one time.
- A recent Wall Street Journal report indicated that insurers received $4.3 billion for Medicaid enrollees simultaneously enrolled in multiple states from 2019 to 2021.
- On July 17, the Centers for Medicare and Medicaid Services (CMS) announced it found 1.2 million people enrolled in multiple state Medicaid programs and 1.6 million people doubly covered by Medicaid and a subsidized exchange plan. CMS estimates that its corrective actions will save $14 billion annually—a massive victory for taxpayers.
- The OBBB requires states to check the Death Master File quarterly to remove deceased Medicaid enrollees and deceased providers.
Background
Under current law, states are supposed to be penalized for improper payment rates above three percent. But this policy has never been enforced; states can receive waivers, permitting waste to continue unabated. The OBBB would limit the ability of the HHS Secretary to waive commonsense, good governance requirements to combat improper payments.
Under the OBBB, there will now be an enforceable budget-neutrality requirement for Medicaid demonstration projects or waivers. States run much of their programs through waivers. Theoretically, this allows states to tailor their programs to the unique needs of their enrollees and test new approaches for the delivery of Medicaid services.
Demonstration projects are supposed to be budget neutral (i.e., not result in more federal spending than would occur absent the waiver). However, lax enforcement and inflated baseline projections often result in demonstrations imposing steep costs on the federal government. The OBBB requires CMS to certify the demonstration’s budget-neutrality requirements for a waiver to be granted.

Get MHF Insights
News and tips for your healthcare freedom.
We never spam you. One-step unsubscribe.
Sponsors

J & DE Family Charitable Fund

Friends
of MHF
Kelly Grotendiek
Philip Harbach
Dale Johnson
Drs. Jeffrey and Joni Jones
Vickie Kahle
Tammy Kipen
Marlin & Kathy Klumpp
Melanie Kurdys
Ruth Nobel
Patrick Peterson
Stephanie Poortenga
Jeanne Smit
Ben and Hope Staal
John Tuinstra
Jacki VanHuis
Sandy Walker
Sign Up for MHF Insights to keep up on the latest in Michigan Health Policy

