







- Built to Serve: The Day That Reminds Us Why We Chose Dentistry

- Journalists Catch You Up on Fauci Hearing, Peptides, and Kids’ Caffeine Consumption

- CMS finalizes 2.3% hospital pay bump, mandatory joint replacement model: 9 things to know
- How ambulatory shifts are reshaping perioperative strategy
- Cyclosporiasis cases top 18,000: 3 updates
- How Allegheny Health Network Strengthened its Foundation for IV Compounding Safety with Automation and Standardization¹
- Health plan customer service reps have AI in their ear
- Centene’s buyouts could have a $315M+ price tag for the rest of the year
- Medicare pay cut sparks specialty battle over skin cancer care
- Cardiovascular Institute of New England provides notice of data incident
- CMS locks in 2.3% inpatient hospital base pay increase, nudges back CJR-X Model start date
- Why autonomy — not just capital — is winning over cardiologists
- The $36 vs. $95 problem: How RVU negotiations are skewing physician pay
- Mississippi hospital board member, former CEO remembered as advocate for rural communities
- Pennsylvania SUD treatment locator reaches 146K users
- Top 10 dental, DSO stories in July
- Ohio youth treatment facility faces scrutiny over reported abuse: 8 notes
- What dental leaders told us in July
- Urban hospital closures and net change, by state
- Nebraska launches dashboard tracking rural health funds
- ADSO sues Colorado Dental Board over practice ownership rule
- New patient acquisition is the top growth driver for dental practices: Report
- 20 new behavioral health projects to know
- Nurses, patients protest North Star Health Alliance ASC closure
- No Surprises Act under attack by payers: 8 things to know
- Dental staffing wages up 23% since 2021: ADA
- AtlantiCare appoints anesthesiology, gastroenterology physician leaders
- Consumer dental spending up 24% over 10 years: 5 stats to know
- Baylor Scott & White joint venture expands outpatient behavioral health services
- 5 DSOs making headlines
- VA to explore GLP-1 treatment for alcohol use disorder: 4 notes
- A $5B wave of M&A hits the ASC industry
- FTC Sues Hims & Hers Over Health Privacy And Billing Practices
- 145 physician medical groups led all healthcare M&A sectors in Q1
- 10 new ASCs in July
- Healthcare exec, telemedicine company owner sentenced for $35M DME fraud scheme
- Amylyx demystifies post-bariatric hypoglycemia with patient education website
- What Dad Eats Before Conception May Influence Baby's Health
- Family History Plays Role In Genetic Risk For Breast Cancer, Researchers Find
- A look at employers' attitudes toward ICHRAs
- Revised 340B Rebate Model Pilot Program moves forward, despite provider pushback
- Function Health lands $450M in growth financing to scale tech-enabled preventive health
- Daiichi Sankyo flags accounting error, as shares tank despite revenue beat
- AbbVie's Skyrizi shrugs off new competition as it thrives in growing psoriasis market
- Op-ed: Hospitals on the edge, a time for CMS to do no harm
- Daily Routine Key To Good Health, Study Says
- Alignment Healthcare boasts 32% revenue jump in Q2, lifts 2026 outlook
- Xpovio mulligan in endometrial cancer comes up short as Karyopharm presses on in myelofibrosis
- Psilocybin Therapy Helps Ease Veterans' Severe PTSD, Pilot Study Finds
- Newsom Reverses On Long-Sought Paid Leave Benefit For California Teachers
- Nicotine Levels Are Rising Among Teens Who Vape, New Study Warns
- The Newest Federally Recognized Tribe Wants Better Healthcare. It May Be On Its Own.

- They Worked To Protect Public Health. Now They Want the Public’s Votes.

- 27 new behavioral health study findings to know
- 21 state behavioral health policy updates
- What will fuel the next wave of DSO growth
- Dentists’ biggest staffing headaches
- Shionogi makes the call on COVID pill Xocova TV spot
- Psilocybin-assisted therapy reduced PTSD symptoms: 3 notes
- Fierce Pharma Asia—Legend CEO exits; Merck’s hush-hush PD-1xVEGF plan; Otsuka’s novel ADHD nod
- Psychedelics, peptides and GLP-1s
- How 'physician-led' care team models tackle primary care's workforce problem
- How 7 systems divert behavioral health patients from the ED
- WellSpan Health, Hippocratic AI ink ‘multi-year’ partnership with plans to co-develop clinical AI agents
- Kaiser faces complaint over automated behavioral health triage system
- Free research hub Nila aims to demystify menopause, other hormone conditions
- Scientists Defend Fauci's Pandemic Work As Senate Hearing Turns Bitter
- Pfizer takes Litfulo to regulators in vitiligo challenge to Incyte, AbbVie
- Study Questions Effectiveness of Antihistamines in Easing Eczema
- Vaping Is Likely Reshaping The Future Of Cancer In The US, Study Argues
- Weekly Rundown: Counsel Health rolls out white label AI care platform; Community Health Network launches MyChart AI assistant
- New CEO Garijo sketches out vision to reverse Sanofi's fortunes as Q2 delivers impressive sales beat
- Alnylam shares tank 29% as Amvuttra disappoints with ATTR outlook cut for 2026
- Waystar boosts 2026 outlook as AI-powered RCM solutions gain traction with providers
- YouTuber MrBeast welcomes Amgen to the channel, kicking off pediatric cancer funding effort
- Booming Dupixent sales fuel Regeneron's biggest quarter since pandemic
- Sugar Consumption Early In Life Linked To Increased Dementia Risk, World War II-Era Data Show
- Work Stress Harming Middle-Age Sleep, Study Says
- RFK Jr.'s Gardasil litigation ties subject to fresh lawmaker scrutiny after Merck settlement
- Bristol Myers delays Cobenfy Alzheimer’s psychosis readout again amid another quarterly beat
- Hospice's Bad Reputation Amid Fraud Crisis Will Hurt Patients, Industry Experts Warn
- Cell Phone Ownership Linked To Lower Reading Skills In Elementary Students
- Listen to the Latest ‘KFF Health News Minute’

- Medicaid Insurers’ Contracts on the Line in Tight Governor’s Race

- Abortion Drug Law in Louisiana Heightens Hemorrhage Risk for Pregnant Patients

- Teladoc Health trims 2026 revenue forecast amid challenges with BetterHelp insurance shift
- Cigna CEO: Express Scripts seeing 'significant early interest' from clients for new rebate-free PBM model
- Viatris runs into FDA roadblock after advertising on-the-go use of cystic fibrosis inhaler
- Sanofi’s new CEO ‘looking deeply’ at late-stage pipeline as clinical clearout continues
- FTC sues Hims & Hers over data privacy, billing practices
- CMS' proposed 340B reimbursement cut—who wins, and who loses?
- Virtual care helps patients improve their gambling disorder symptoms, Birches Health finds
- Case Western Reserve University launches next-generation healthcare leadership program
- Lilly, Resilience commit $750M to boost US diabetes, obesity med production
- CMS ending Medicare Part D subsidy program
- Red Cross Declares Rare National Blood Supply Crisis Amid Summer Shortfall
- Not Just Pregnancy Fatigue: Could It Be Sleep Apnea?
- More Women Drinking During Pregnancy
- Wellstar Health System lays off 761 corporate, administrative staff
- Biogen flips '26 guidance from expected decline to sales increase
- Teva’s innovation engine offsets generics slump, leaving one analyst ‘shocked’ by Ajovy’s surge
- Talking To Your Baby? Eye Contact Is Key To Language Development, Experiment Shows
- Boosted by CMS settlement, Incyte expects Opzelura to cross $1B in 2026
- Leapfrog launches expanded ASC public reporting program
- Cyclospora Boosts Fears That Deadlier Foodborne Outbreaks Are Ahead
- DoorDash, GrubHub Delivering Junk Food To 1 In 4 Teens During School Hours
- Uninsured but Undaunted, a Surgical Patient Searched the Globe for a Deal

- Trump Has Quietly Throttled an Agency Devoted to the Safety of American Healthcare

- Hospice’s Bad Reputation Amid Fraud Crisis Will Hurt Patients, Industry Experts Warn

- Humana plans more market exits for 2027, CFO says
- PMCPA sanctions melatonin drugmaker over misleading information
- CG Life embraces next-gen era in merger with AI-native agency The Considered+AI
- How 2 FDA citations complicate Hengrui, Elevar’s push for liver cancer combo approval
- Fifth Death Reported In NYC Legionnaires' Disease Outbreak
- Many Young Adults Aren't Ready To Manage Their Own Healthcare, Poll Finds
- Can A Daily Multivitamin Help You Stay Active As You Age?
- Stellarus launches AI-powered health plan customer service representative copilot
- Prebiotic Soda Health Claims Questioned In New Nutrition Study
- Family-Based Childhood Obesity Program Helps Kids Cut Weight, Become Healthier
- To Afford Aging In Place, Older Adults Turn To 'Golden Girls' Housing
- Breakfast Can Help Teens Make Better Food Choices Throughout Their Day, Study Says
- Newsom Reverses on Long-Sought Paid Leave Benefit for Teachers in California

- FDA Panel Backs Two Peptides For Compounding, Rejects One
- How Accurate Are Photo-Based Calorie Apps? 4 Are Put To The Test
- Popular School Cafeteria Meals Need An Update To Meet Healthy Food Standards, Researchers Say
- Ovarian Syndrome Quadruples Heart Disease Risk In Women, Major Study Concludes
- Weed-Killing Chemical, Glyphosate, Linked To Premature Births In Humans, Study Says
- 'The Child Is Terrified': Doctors On Front Lines Of Measles Comeback Speak Out
- 'Yo-yo' Weight Loss Linked To Decline In Muscle Mass
- FDA Advisers Dismiss Safety Warnings, Back Four Peptide Treatments
- Frequent Marijuana Use Linked To Higher Stress Hormone Levels
- Back Pain? Try Swimming, Study Says
- Ozempic Cuts Down Calorie Intake For At Least A Year, Even If Hunger Returns, Trial Finds
- Money Problems Might Make Your Brain Old Before Its Time, Study Suggests
- Black MS Patients Dying Younger Than White Ones, Study Finds
- Headstands and Summervaults: A Statement on Crypto Vaults and Lending Strategies
- Remarks at the Small Business Capital Formation Advisory Committee Meeting
- Seeking Public Comment on Seeking Public Capital: Remarks Before the Small Business Capital Formation Advisory Committee
- Remarks to the Small Business Capital Formation Advisory Committee
- Statement on Regulation E-Delivery
- Paper Taper: Statement on Proposed Regulation E-Delivery
- Statement on Proposed Regulation E-Delivery
- Senate HELP committee advances nominees for CDC director, HHS preparedness head
- Remarks before the American-Hellenic Chamber of Commerce
- Remarks at the Society for Corporate Governance Conference
- Zimmer Biomet to Hire 500 in India as New Bengaluru Technology Centre Drives AI and MedTech Innovation
- Zimmer Biomet to Hire 500 in India as New Bengaluru Technology Centre Drives AI and MedTech Innovation
- AdaptHealth Investigates Data Breach After Social Engineering Attack, Possible Link to ShinyHunters Emerges
- AdaptHealth Investigates Data Breach After Social Engineering Attack, Possible Link to ShinyHunters Emerges
- Statement on the 2026 Regulatory Agenda
Michigan healthcare freedom community forum

I am so old I can remember when the media told us no illegal immigrants were receiving Medicaid benefits. HHS' Centers for Medicare and Medicaid Services (CMS) is giving Immigration and DHS Immigration and Customs Enforcement (ICE) officials access to the personal data of 79 million Medicaid enrollees. The screaming in your left ear has just begun:
US health department hands over Medicaid personal data to ICE
By Ahmed Aboulenein and Kanishka Singh - July 17, 2025WASHINGTON, July 17 (Reuters) - The U.S. health department is giving Immigration and Customs Enforcement officials access to the personal data of 79 million Medicaid enrollees to help them track down immigrants who may not be living legally in the country, it said on Thursday.
Giving ICE access to the personal data of Medicaid enrollees marks an escalation in President Donald Trump's hardline immigration policies. It may also raise privacy concerns under the Health Insurance Portability and Accountability Act, known as HIPAA.
A Department of Health and Human Services spokesperson said sharing data between the Centers for Medicare and Medicaid Services and the Department of Homeland Security, which oversees ICE, fell within the department's legal authority.
"With respect to the recent data sharing between CMS and DHS, HHS acted entirely within its legal authority – and in full compliance with all applicable laws – to ensure that Medicaid benefits are reserved for individuals who are lawfully entitled to receive them," the spokesperson said.
A spokesperson for the Department of Homeland Security said the department was exploring an initiative with CMS to ensure people living in the country illegally do not receive Medicaid benefits.
The agreement was first reported earlier on Thursday by the Associated Press, which said it was signed on Monday.
The Medicaid health program for low income people is jointly funded by the federal government and states.
Immigrants who are in the U.S. illegally are not eligible for Medicaid under federal law, but 14 states and the District of Columbia provide coverage for eligible children regardless of immigration status, and seven states and DC do so for adults.
"CMS is aggressively cracking down on states that may be misusing federal Medicaid funds to subsidize care for illegal immigrants. This oversight effort – supported by lawful interagency data sharing with DHS – is focused on identifying waste, fraud, and systemic abuse," the HHS spokesperson said.
The spokesperson did not address questions from Reuters on the type of data being shared or on how HHS would ensure HIPAA protections are upheld. The AP, citing a copy of the data sharing agreement, said the data included home addresses and ethnicities.
The agreement is the latest in a series of moves by the health department in support of the Trump administration's immigration crackdown and comes a week after it widened its interpretation of a law banning most immigrants from receiving federal public benefits.

AMAC drew ICE a nice roadmap in May.
Democrats Forced to Reckon with Reality on Healthcare for Illegal Aliens
May 29, 2025For years, Democrats have touted “Medicare for all” as a sacred mantra, no matter the price tag or who foots the bill. Now, deep-blue states are finding out the true cost of such virtue signaling.
In the most recent development, news broke last week that Illinois Governor JB Pritzker’s latest budget proposal cuts funding for a program that provides taxpayer-funded healthcare to illegal aliens aged 42 to 65. Democrats in Springfield are unsurprisingly outraged over the proposed cut, but as Pritzker’s office made clear, the math simply doesn’t add up. The program is expected to cost about $538 million this year alone – even as the state faces a soaring budget deficit.
But as disastrous as taxpayer-funded healthcare for illegal aliens has been in Illinois, things are even worse in California and Minnesota, which both rolled out programs offering “free” healthcare to every illegal alien, regardless of age. California Governor Gavin Newsom, once the policy’s biggest champion, is now freezing new enrollments as costs spiral. Meanwhile, Minnesota Democrats are publicly battling over their runaway Medicaid expansion.
As AMAC reported last month, California’s journey into this mess began in 2022, when Newsom and the Democrat supermajority extended Medi-Cal, the state’s Medicaid program, to all adults aged 26 to 49, regardless of immigration status. The move, which took effect in 2024, was billed as a national first and, in Newsom’s words, a “transformative step towards strengthening the healthcare system for all Californians.”
Officials initially estimated about 764,000 illegal immigrants would enroll. Instead, enrollment has been roughly 1.6 million and continues climbing, according to CalMatters. The state is now scrambling for billions to cover these colossal miscalculations. Newsom has resorted to taking out $6.2 billion in loans from the general fund to keep Medicaid afloat.
As AMAC Newsline recently noted, this isn’t really a loan – it’s a bailout. With California’s debt already at $273 billion, Medi-Cal is unlikely to repay the general fund. Newsom’s choice to prioritize illegal aliens over taxpaying citizens has drawn harsh criticism from California Republicans, who called for a freeze on new enrollments. But thanks to a Biden-era policy, California Democrats have used a deceptive maneuver to pass the bill off to federal taxpayers.
In essence, California can tax Medicaid insurers, then pay that money back to those same insurers through Medicaid payments for patient care. This artificially inflates the state’s Medicaid spending on paper, which means California qualifies for a larger federal match, effectively turning state-collected tax dollars into extra federal funding.
In practice, this means federal taxpayers everywhere – blue state, red state, doesn’t matter – are paying billions each year to prop up California’s Medicaid expansion for illegal aliens. Still, California’s spending problem couldn’t be hidden forever. Newsom is now desperately trying to slow the bleeding, according to National Review.
Starting next year, the state will stop enrolling new low-income illegal aliens in Medi-Cal. Coverage won’t be stripped from those already enrolled, but new applicants will be denied. By 2027, adults with “unsatisfactory immigration status” must pay a $100 monthly premium.
The about-face should hardly be a surprise after the program blew through cost projections by $2.7 billion, with Newsom acknowledging the need for “difficult but necessary steps” to preserve Medi-Cal’s fiscal viability. His office estimates that freezing new enrollments and adding premiums could save $5.4 billion by 2028-29.
It’s important to note these “savings” don’t mean California will recover or bank $5.4 billion. Instead, the figure reflects money the state will avoid spending compared to what projections had been had the program continued unchecked. In other words, these are costs California won’t incur, not funds returning to the budget.
Minnesota followed California’s lead into financial ruin, launching a similar plan expecting 5,700 illegal alien enrollees. Instead, over 20,000 signed up within months, pushing costs nearly 30 percent over budget and climbing, according to Conservative Brief. The state’s response was to end coverage for undocumented adults while allowing children to remain on the rolls.
Even though Minnesota Governor Tim Walz himself admitted spending is unsustainable, the cuts predictably sparked left-wing outrage elsewhere.
State Senator Alice Mann accused Republicans of trying to strip people of their healthcare “under the guise of fiscal responsibility.” But as Republican House Speaker Lisa Demuth noted, “Those that are here illegally, they can still join the private market, so it’s not that healthcare is being denied in any way.”
What’s happening in California and Minnesota isn’t a fluke. It’s the natural endgame of the Democrat Party’s open-borders, free-healthcare-for-all agenda. The left refuses to accept one simple truth – there’s always a price, no matter how noble the cause. Vague overtures to “compassion” and “kindness” don’t balance budgets, and every “free” service they promise shifts the cost onto someone else.
In the end, it’s not just the taxpayers of Illinois, California, and Minnesota left dealing with the hangover; every American taxpayer must pick up the tab. Democrats are running out of places to hide from the fallout of their own policies. The question is whether voters will let them try the same playbook on a national scale or if these state-level fiascoes will serve as a warning enough.
Sarah Katherine Sisk is a proud Hillsdale College alumna and a master’s student in economics at George Mason University.
AG Nessel, among 19 other state AGs, succeeded in blocking DHS access to illegal immigrant Medicaid records.
Health IT report:
https://www.healthcareitnews.com/news/use-medicaid-data-ice-blocked-20-states
Use of Medicaid data by ICE blocked in 20 states
The Department of Homeland Security may not use Medicaid data for immigration enforcement purposes and the Department of Health and Human Services may not share the protected patient information, according to a federal court ruling.
By Andrea Fox | August 18, 2025
ICE's access to that medical data has raised concerns that individuals may avoid seeking necessary care out of fear their private information would be shared – compromising public health and potentially increasing states' healthcare costs.
That prompted a multistate lawsuit, which has led to the Department of Homeland Security being precluded from using the Center for Medicaid & Medicare Services' data obtained for immigration enforcement purposes.
That includes data already acquired, until the termination of this litigation or 14 days after DHS and the Department of Health and Human Services complete "a reasoned decisionmaking process," according to the judge's ruling.
WHY IT MATTERS
In the complaint brought against President Donald Trump’s administration last month in Northern California federal court, attorney generals from 20 states – California, Arizona, Colorado, Connecticut, Delaware, Hawaii, Illinois, Maine, Maryland, Massachusetts, Michigan, Minnesota, Nevada, New Jersey, New Mexico, New York, Oregon, Rhode Island, Vermont and Washington – sought to bar use of Medicaid data for immigration enforcement and deportation purposes.
The attorneys general argued that the administration "abruptly changed, without notice, opportunity for public input, or reasoned decision-making" its policy of keeping state Medicaid agencies’ healthcare records confidential in their lawsuit filed July 1.
Because ICE had a policy against using Medicaid data for immigration enforcement purposes, which had been publicized to states, medical providers and Medicaid patients since 2013, U.S. District Judge Vince Chhabria said he would grant them a partial preliminary injunction.
Medicaid data from several states, which could include Children’s Health Insurance Program data, was shared with ICE officials, according to the complaint.
That action, they argued, would compromise the health of individuals experiencing emergencies and leave states and their safety net hospitals footing the bill for federally mandated emergency healthcare services.
"If members of our community cannot trust that the government will keep their medical history and other personal data safe, they will think twice about going to the doctor when needed," the attorneys general said.
"Congress itself extended coverage and federal funds for emergency Medicaid to all individuals residing in the United States, even those who lack satisfactory immigration status," they noted.
They also asked for immediate relief to protect state data and "to bar the federal government from reneging on the terms of the longstanding State/federal Medicaid partnership," and the judge agreed the attorneys proved their claims that the federal decision to share the PII was arbitrary and capricious.
"It appears that ICE is primarily focused on obtaining current address information for people who are in the country unlawfully," Chhabria wrote. "But CMS appears to have granted ICE unfettered access to all information about all Medicaid patients in the United States, whether citizens or noncitizens."
However, Chhabria denied the plaintiffs' request to require the federal agencies to undertake notice-and-comment rulemaking before deciding whether to change their policies because "several federal statutes appear to permit, and sometimes even require, agencies to provide such information to DHS upon request."
THE LARGER TREND
As part of Trump's executive order, Ending Taxpayer Subsidization of Open Borders, CMS said in May that it would crack down on Medicaid funding for immigrants and act "decisively" to ensure funds are used for eligible individuals only.
Then in June, federal health agency staff were asked to release personally identifiable information for Medicaid enrollees in seven states – California, New York, Washington, Oregon, Illinois, Minnesota and Colorado – that permit non-U.S. citizens to enroll.
All U.S. states are required to offer temporary emergency Medicaid coverage that pays just for lifesaving services in emergency rooms to anyone, including non-U.S. citizens, who are lawfully present or not.
But ICE was provided access to the personal data of the 79 million Medicaid enrollees to help track down immigrants who may not be living legally in the United States, according to a data-sharing agreement between CMS and DHS reportedly obtained by The Associated Press in mid-July.
That agreement allowed ICE to access the data between 9 a.m. and 5 p.m., Monday through Friday, through Sept. 9.
"It’s unthinkable that CMS would violate the trust of Medicaid enrollees in this way," Hannah Katch, a former CMS adviser, had told the AP.
ON THE RECORD
"Everyone should be able to seek medical care without fear of what the federal government may do with that information," said Nick Brown, attorney general of Washington state, in a statement following the injunction.
Gov. Whitmer's response this morning, via MDHHS email to Michigan providers.
All Providers,
The purpose of this communication is to inform all Medicaid Providers that the United States Department of Health and Human Services (USDHHS), including the Centers for Medicare & Medicaid Services (CMS), is currently prohibited by a preliminary injunction from sharing Michigan’s Medicaid data with the Department of Homeland Security (DHS), for immigration enforcement purposes. Michigan Department of Health and Human Services (MDHHS) has become aware that some Medicaid providers have raised questions and concerns about the recent notices and actions of USDHHS, CMS, and DHS related to demands for and potential use of beneficiary-level State Medicaid data being shared with DHS’ Immigration and Customs Enforcement (ICE). A hearing is scheduled for December 9, 2025, related to whether USDHHS, CMS, and DHS will continue to be prohibited from using Michigan’s state Medicaid data for immigration enforcement purposes. MDHHS will provide further notice if there are changes to what is considered permissible use, disclosure, or sharing of Michigan’s Medicaid data by USDHHS or CMS because of this hearing.
🤔 I am so old I remember being told that illegal immigrants never receive Medicaid benefits. 🤔
#MeToo.
Just last month, in fact: a die-hard response to my letter (with citations) in the local paper!
There's no doubt on which side the administrative state falls on this question.
MDHHS today, via email:
All Providers,
The purpose of this communication is to inform all Medicaid Providers that the United States Department of Health and Human Services (USDHHS), including the Centers for Medicare & Medicaid Services (CMS), is currently prohibited by a preliminary injunction, that has been extended through January 5, 2026, from sharing Michigan’s Medicaid data with the Department of Homeland Security (DHS), for immigration enforcement purposes. Michigan Department of Health and Human Services (MDHHS) has become aware that some Medicaid providers have raised questions and concerns about the recent notices and actions of USDHHS, CMS, and DHS related to beneficiary-level State Medicaid data being shared with DHS’ Immigration and Customs Enforcement (ICE).
MDHHS will provide further notice if there are changes to what is considered permissible use, disclosure, or sharing of Michigan’s Medicaid data by USDHHS or CMS because of any future court actions.
AG Dana Nessel and her secret cabal of Democratic Attorneys General lost in District Court. Obama Judge Vince Chhabria just ruled that ICE officials can access basic personal information of Medicaid recipients. Of course nothing will be found, because illegal aliens have no access to Medicaid benefits - right? Right? RIGHT?
Judge rules Trump admin can share illegal migrant Medicaid data with ICE
U.S. District Judge Vince Chhabria ruled that ICE officials can access six categories of “basic” personal information: Address, citizenship, immigration status, phone number, date of birth and Medicaid ID.
By Misty Severi - December 29, 2025A federal judge ruled Monday that the Trump administration can share Medicaid information pertaining to illegal migrants with Immigration and Customs Enforcement officers next month.
The ruling comes after 22 Democratic states sued to stop the government from sharing the information in July, which was granted while the case played out. The liberal states can still appeal the ruling.
The order approved an agreement between the Centers for Medicare and Medicaid Services and the Department of Homeland Security in July that allowed ICE officials to access the personal data of 79 million Medicaid enrollees, including home addresses, to track down the illegal migrants.
U.S. District Judge Vince Chhabria ruled that ICE officials can access six categories of “basic” personal information: Address, citizenship, immigration status, phone number, date of birth and Medicaid ID.
“The sharing of such information is clearly authorized by law and the agencies have adequately explained their decisions,” Chhabria wrote in the seven-page order. “Beyond the basic information discussed above, the policies are totally unclear and do not appear to be the product of a coherent decision-making process."
The order, which is limited to migrants known to be in the country illegally, comes because seven blue states allow migrants to receive state funds through their respective Medicaid programs, but not federal ones.
The seven blue states are: California, Colorado, Illinois, Minnesota, New York, Oregon and Washington.
This is nothing new. The states all KNEW that when the Marketplace was being set up, the Feds were only going to fund it for 3 years. After the 3 years were up, the states were going to have to find the means to fund it themselves. The states brought this on themselves and tried to fix the problems on the backs of the taxpayers. They forgot that with federal dollars come federal strings...and HUGE increases for people once the subsidies were gone.
@cj1954 you know it.
if they didn't know, they should have. Still, Michigan legislators at the time claimed that the feds promised full ongoing Healthy Michigan funding.
Then, those same legislators appeased voter concerns by putting the conditional "drop-out" clause in so that "Michigan would never be on the hook for expanded Medicaid."
Phase 3 was predictable. Last term, Michigan legislators repealed the drop-out clause. (As they did the able-bodied work requirement.)
So my question is: back in the day, were pro-expansion legislators forgetful, ignorant, or just overcome by wishful thinking with the dollar signs in their eyes?
We noted this in the HOTLINE several weeks ago with our back of the envelope math. Now, we have validation from Johns Hopkins Professor Ge Bai and TCU Professor Elizabeth Plummer in the WSJ:
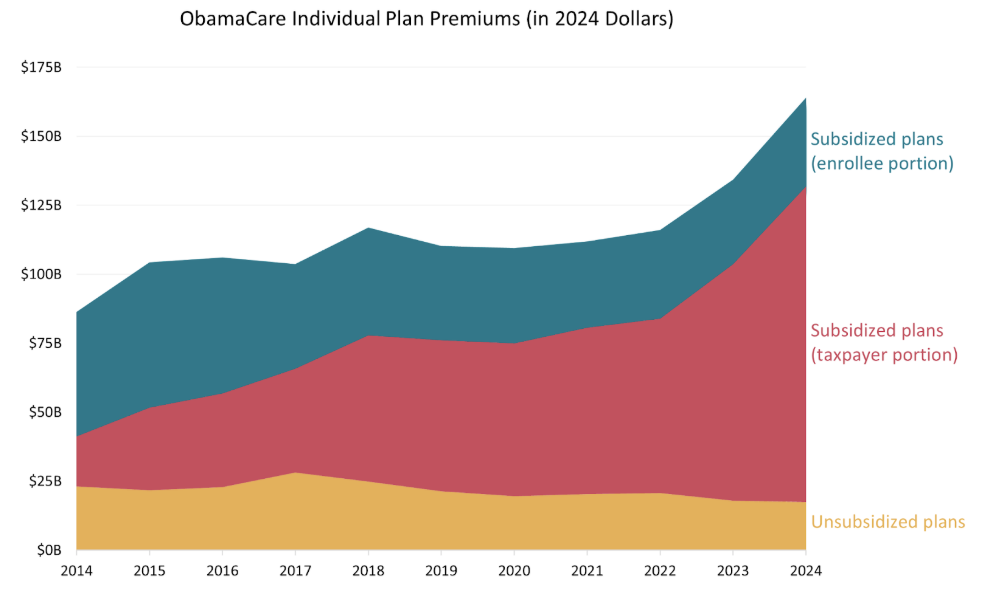
Using health insurers’ mandatory filings, our study, published Friday in JAMA Health Forum, shows that the ObamaCare individual market has become a money pit for taxpayers. In 2024 they paid nearly 80% of the premiums for subsidized plans–compared with only 30% in 2014.
Taxpayers paid more than $114 billion directly to insurers in 2024–one-third more after inflation than in 2023, more than double the amount in 2020 (before the enhanced subsidies), and more than six times as much as in 2014. According to the Congressional Budget Office, this acceleration continued in 2025.
The chart below from https://jamanetwork.com/journals/jama-health-forum/fullarticle/2843117&source=gmail&ust=1767193329240000&usg=AOvVaw2y3GX69VMzDoDACrJMbDV u">the JAMA study shows that premiums have exploded in plans that receive subsidies and the increase was entirely at taxpayer expense. That is the red portion of the chart. But premiums have been flat in unsubsidized plans.
There’s an economic lesson here: if you subsidize something, you get more of it.
300w,
768w,
370w,
760w,
570w" data-eio-rwidth="986" data-eio-rheight="608" />

The story of California's illegal immigrants on Medicaid. A $ 19 billion drain on federal taxpayers:
Medicaid, ICE and a ticking clock for undocumented Californians
An enrollment freeze and immigration officials’ push to access health data are forcing undocumented Californians to weigh free health care against deportation risks.
By Rachel Bluth - January 1, 2026SACRAMENTO, California — As 2024 came to a close, Mar Velez and her team of outreach workers were fanned out across California, signing undocumented immigrants up for Medi-Cal, the state’s health insurance program. They made a compelling, straight-forward offer: It’s free, no questions asked.
A year later, that pitch was much more complicated — and the stakes far higher.
They were, for one, racing against the clock to enroll people before Jan. 1, when a cost-saving freeze on new enrollments imposed by the state took hold. But, at the same time, there was a new risk that cames with enrolling as the Trump administration seeks to use personal information collected by states to find and deport immigrants who are in the country illegally.
“We live in a new reality,” said Velez, the director of policy at the Latino Coalition For A Healthy California, a group that advocates for health policy in Sacramento and funds community health workers on the ground. “The things we could rely on before aren’t there anymore.”
California first offered Medi-Cal to some undocumented children in 2016 and expanded the program gradually until 2024, when immigrants of all ages who met income requirements were able to enroll regardless of immigration status.
That final expansion blew up the state’s budget, costing almost $3 billion more than anticipated. Gov. Gavin Newsom and Democratic lawmakers scaled back the ambitious program this year with the enrollment freeze and $30 monthly premiums for undocumented immigrants already in the program that start in 2027, which together are expected to reduce costs by about $78 million in the first year and up to $3.3 billion by 2029.
The fallout from those moves will be significant as the freeze and premiums are projected to cause the number of people enrolled in Medi-Cal to fall by 1.5 million by 2030.
The Trump Administration has injected uncertainty and risk into the equation with its crackdown on illegal immigration. To help identify and deport undocumented immigrants, the administration wants ICE agents to have access to information California and other Democratic-led states collect on people enrolled in their health insurance programs. After it was revealed in June that some data had been shared, the states sued and a judge temporarily barred the government from continuing with the practice.
Trump officials made clear in November that they intend to resume the data sharing as soon as possible and earlier this month a federal judge indicated he may allow them to do so.
The fight over the legality of the data sharing won’t be resolved until after the start of the new year, leaving undocumented immigrants in California with a stark choice to forgo free health care or roll the dice that signing up for Medi-Cal won’t bring ICE agents to their door.
Some people have moved so they’re no longer at the address they used to register for Medi-Cal, Velez said.
Instead of cheerleading for enrollment, the Spanish-speaking workers Velez has dispatched around the state, who are called promotoras de salud, say they’re being more neutral. They provide information about registration deadlines, what personal information is needed to enroll, and how that data could be shared.
“These are your rights, and these are the risks,” Lisbet Ruiz, a promotora in San Diego said she tells her clients. “But at the end of the day, we don’t tell them to make a decision.”
The stakes are high, and promotoras are keeping their opinions to themselves on whether or not it’s too risky to enroll. The best they can do is empower people with information, Ruiz said.
There’s also fear among Ruiz’s clients over the “public charge rule,” a proposal from the Trump Administration to consider the amount of public services a person has used when evaluating their application for residency or citizenship. Though the rule isn’t yet in effect, the fear of it one day coming to pass is keeping people from enrolling in Medi-Cal, Ruiz said.
Ruiz recalled a woman who was in the U.S. on a visa issued to people fleeing domestic violence who was afraid to get services for herself or her autistic son. Despite Ruiz’s assurances that taking food benefits or Medi-Cal for her and her autistic son was unlikely to hurt her chances of being able to remain in the country, the woman refused.
“She still made the decision not to get into it because of the risk,” Ruiz said.
Despite the turmoil, some counties and nonprofits are aggressively pushing enrollment before the freeze sets in. In Santa Clara, the county earmarked $2.5 million for an outreach and enrollment campaign, especially for the undocumented population.
“We don’t want [undocumented] people…to forever lose their access to health care,” said Nikki Fortunado Bas, a county supervisor.
Community health workers in San Jose are working with the county on outreach. Darcie Green, executive director of Latinas Contra Cancer, a health advocacy group in the county, said there’s an “immediate need” to get people re-enrolled or enrolled for the first time before they lose eligibility.
Green said she’s trying to quell fears while still being realistic with people and encouraging them to get care.
“These are conversations we’re going to continue having, but the directive we have right now from our county and our clinic system is that we’re still encouraging people to enroll,” she said.
And many are balancing the threat of immigration enforcement against their need for prenatal care, prescription medications or other medical services this year. Karem Martinez is the enrollment lead at East Valley Community Health Center, a clinic that serves Pomona, Covina, West Covina and El Monte.
At her clinic, people are less afraid of immigration enforcement now than earlier this year when ICE had a major presence in Los Angeles. She said people took the looming enrollment freeze seriously. Some of her clients have come in with pay stubs every month trying to see if their income is low enough to qualify.
Patricia Lopez, the manager of the health insurance program at the Venice Family Clinic is seeing similar decisions play out in real time.
A woman recently came to Lopez after allowing her Medi-Cal coverage to lapse.
Worried about immigration enforcement, the woman had decided to go without health insurance but then sought Lopez’s help when she realized she couldn’t afford her medication.
Lopez said she reminded the woman that in the new year she would be shut out from re-enrolling forever if she let her coverage lapse again.
Lopez said that in previous years she typically had 30 or 40 people coming in for help with insurance during each three-hour walk in window, and that these days the number is in the teens. Clinics don’t collect information on a client’s immigration status, so there’s no way of knowing how much of the decline is among citizens or the undocumented population.
Minisinformation and misunderstanding is common, making it even harder to get people enrolled, advocates said. People think the freeze and premiums have already started, or that come January everyone will get kicked off the program.
For now, Velez said she’s trying to get the message out that there’s still time to sign up, but she’s being realistic about the risks associated with Medi-Cal.
“It’s hard to deliver that kind of information to communities,” Velez said. “But if we’re not doing that, we aren’t doing our jobs.”
Get MHF Insights
News and tips for your healthcare freedom.
We never spam you. One-step unsubscribe.
Sponsors

J & DE Family Charitable Fund

Friends
of MHF
Kelly Grotendiek
Philip Harbach
Dale Johnson
Drs. Jeffrey and Joni Jones
Vickie Kahle
Tammy Kipen
Marlin & Kathy Klumpp
Melanie Kurdys
Ruth Nobel
Patrick Peterson
Stephanie Poortenga
Jeanne Smit
Ben and Hope Staal
John Tuinstra
Jacki VanHuis
Sandy Walker
Sign Up for MHF Insights to keep up on the latest in Michigan Health Policy

